Calvarial Reconstruction With Split Rib Grafts
David A. Staffenberg
Gerald J. Cho
DEFINITION
The rib cage is made up of paired ribs, sternum, and thoracic vertebrae acting to protect and stabilize the chest cavity.
Because the rib cage is comprised of 24 ribs and resection of as many as 2 ribs is well tolerated (ie, does not cause chest wall instability), the rib cage is an abundant source of bone graft material.
ANATOMY
The rib cage or the thoracic cage consists of bone and cartilage.
Normally, there are 12 ribs on each side. Each rib articulates with the thoracic vertebral column posteriorly, and the first 10 ribs articulate with the sternum via the costal cartilage.
The caudal two ribs are “floating ribs” and lack corresponding costal cartilages (FIG 1).
Rib grafts are technically easier and safer to obtain than split calvarial grafts in children below the age of 8 because the diploe of the calvarium at this age is poorly developed. Moreover, unlike the iliac crest donor site, rib graft harvest is less painful and does not affect growth potential of the pelvis.
The rib is circumferentially surrounded by cortical bone and has a cancellous core. The rib can be split into two mirror images to increase the surface area.
Splitting the bone also makes it more malleable to match the cranial contour.
 FIG 1 • The rib cage. Normally, there are 12 ribs on each side. The caudal two ribs are “floating ribs” and lack corresponding costal cartilages. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Patient history and physical exam should document prior history of chest surgery or trauma particularly previous scars and their location, as well as history of prior rib graft harvest.
IMAGING
Preoperative chest x-rays are rarely necessary prior to harvesting of rib grafts unless there is an unusual finding on physical exam.
Similarly, postoperative chest x-rays are usually unnecessary even if there is a small violation of the parietal pleura as this rarely leads to a clinically significant pneumothorax. If there is suspicion of injury to the visceral pleura or lung parenchyma, then a chest x-ray and close clinical observation may be warranted.
SURGICAL MANAGEMENT
Preoperative Planning
Skin incisions are marked along the relaxed skin tension lines to minimize postoperative scarring.
In females, an inframammary fold incision may be used and is located at approximately the level of the fifth rib.
Incisions are placed lateral to the costochondral junction to avoid harvesting of the costal cartilage, which is not useful for calvarial reconstruction.
The length of the incision is related to the amount of bone that is necessary. Nevertheless, it is possible to minimize the length of the incision with the use of angled Horsley rib cutters.
Harvesting of more than two adjacent ribs should be avoided to minimize the risk of flail chest and respiratory compromise.
Positioning
The patient can be positioned prone or supine as rib harvest is possible from both the anterior and posterior chest.
The choice for positioning depends largely on the cranioplasty defect to be treated and aiming to avoid repositioning during surgery.
TECHNIQUES
▪ Rib Graft Harvest
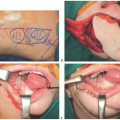
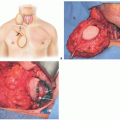
The skin is incised and dissection is carried down to the anterior rectus fascia for the anterior approach. The fascia and muscle are split along the underlying rib using careful palpating as a guide (TECH FIG 1A).
The periosteum of the rib is elevated along the length of the bone using Freer or Joseph elevators.
Care is directed at the inferior border of each rib where the neuromuscular bundle lays under a small overhang. The neuromuscular bundle is carefully preserved.
A Doyen elevator (available in pediatric and adult sizes) is used to continue periosteal dissection under the rib and extend the dissection laterally.
It is most advantageous to first separate the bony rib from the costal cartilage (in the anterior approach) or to use a scalpel to divide the cartilage just medial to the junction while a malleable retractor protects the underlying periosteum and pleura (TECH FIG 1B).Related posts:
 Lateral Mandible Reconstruction With Soft Tissue Flaps
Lateral Mandible Reconstruction With Soft Tissue Flaps
 Repair of Lip Defects With Karapandzic Flaps
Repair of Lip Defects With Karapandzic Flaps
 Lower Eyelid Reconstruction With Palatal Grafts
Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


