Fig. 18.1
Anatomy of the great saphenous vein Reproduction of a lithograph plate from Gray’s anatomy (Henry Gray, Anatomy: Descriptive and Surgical)
It originates from where the dorsal vein of the first digit (the large toe) merges with the dorsal venous arch of the foot. After passing anterior to the medial malleolus (where it often can be visualized and palpated), it runs up the medial side of the leg.
At the knee, it runs over the posterior border of the medial epicondyle of the femur bone.
The small saphenous vein is a relatively large vein of the superficial posterior leg.
Its origin is where the dorsal vein of the fifth digit (smallest toe) merges with the dorsal venous arch of the foot, which attaches to the great saphenous vein. It is considered a superficial vein and is subcutaneous (just under the skin).
From its origin, it courses around the lateral aspect of the foot (inferior and posterior to the lateral malleolus), runs along the posterior aspect of the leg, passes between the heads of the gastrocnemius muscle, and usually drains into the popliteal vein approximately at or above the level of the knee joint.
Accidental injury to saphenous veins leads to noticeable hematomas and blood infarction of the implant with possible infection.
18.2 Pitfalls
Identification of the saphenous veins must be accomplished prior to injecting the filler by means of visual, tactile, and echographic examination (Figs. 18.2, 18.3, 18.4).

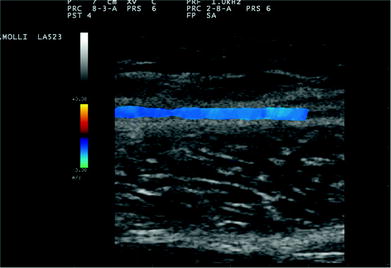

Fig. 18.2
Ultrasound examination is performed in order to design the course of saphenous vein
Fig. 18.3
Ultrasound Doppler image of saphenous vein
Fig. 18.4
Design of saphenous vein course
The injecting cannula must be directed into the subcutaneous layer, keeping the hedge superficial to the muscularis fascia of the gastrocnemius.
The point and area of injection must be decided according to the defect to be corrected.
18.3 Calves Augmentation with Hyaluronic Acid
Augmentation of the calves by hyaluronic acid is a simple procedure, performed in the office operating room under local anesthesia.
18.3.1 Indications
Augmentation of the calves to improve harmony of the legs.
18.3.2 Contraindications
The filler should not be injected in areas that lack sufficient blood supply or that have an infection or inflammation.
No injection should be done if the hand has been previously treated with liquid silicone or other permanent fillers because new injection could lead to inflammation or infection of the implants.
Any hypersensitivity to any components of the filler obviously constitutes a contraindication for the treatment.
Vascular problems as arterial or venous occlusion are relative contra-indications that must be evaluated by a specialist before treatment.
18.3.3 Operating Time
The procedure usually takes 30–60 min.
18.3.4 Materials
Usually, the procedure is performed using from 20 to 120 cc of hyaluronic acid and Macrolane VRF20 or Hyacorp 500 (from 10 to 60 cc injected in one calf) (Figs. 18.5, 18.6a, b, c).

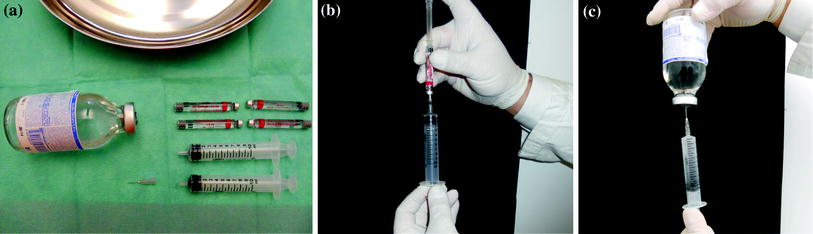
Fig. 18.5
Calves augmentation by hyaluronic acid: Materials
Fig. 18.6
a, b, c Preparation of anesthesia. Anesthetic solution is made up by mixing 6.4 ml of physiologic solution with 3.6 ml of mepivacaine (20 mg/ml) with epinephrine (1/100000)
Blade number 15
Sharp scissors
Hudson forceps
Small Kleimer
2.5 × 150 mm, 12 G, filling cannula
3 × 10 cc syringes
1 × 100 cc bottle of physiologic solution.
18.3.5 Material Choice
Macrolane VRF 20
Macrolane VRF 30
Hyacorp 500
Hyacorp 1000
18.3.6 Methods
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


