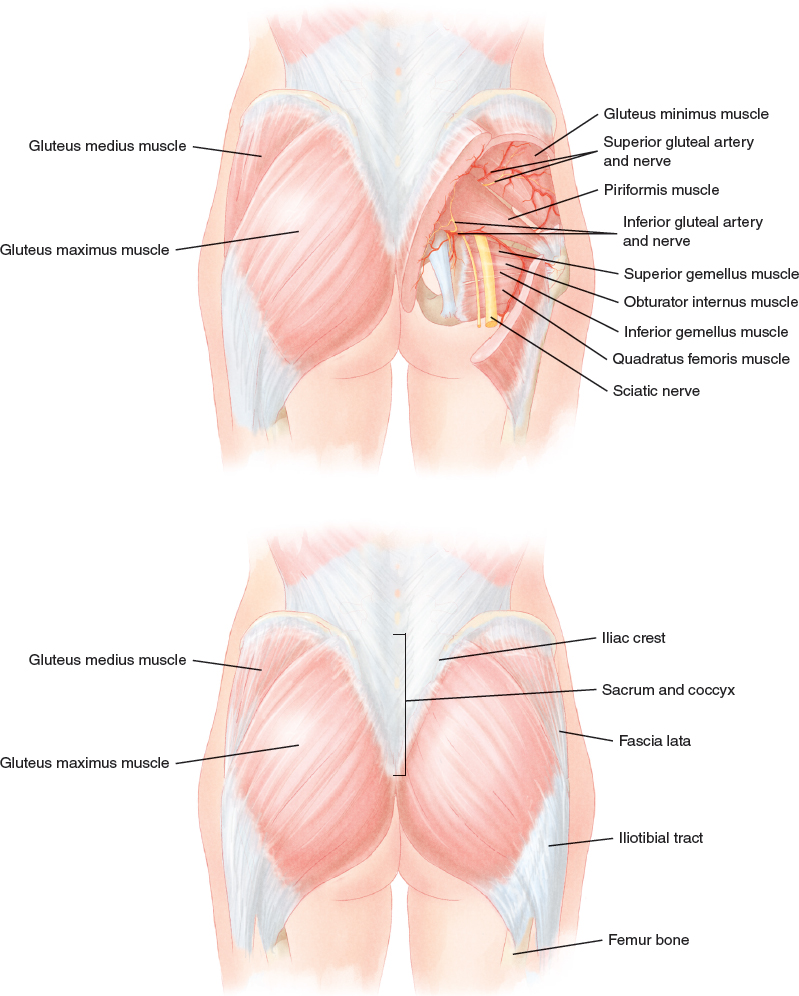
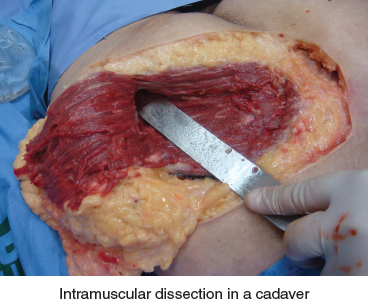
CHAPTER 18 José Horácio Aboudib Early examples of art indicate that interest in the human figure, and specifically the female body, was initially focused on the breasts and vulva. The Greeks and Romans emphasized fleshy, rounded buttocks as a symbol of fertility, youth, and beauty. Fig. 18-1 An example of this fascination with the shape of the buttocks is demonstrated in the statue of Aphrodite, the Callipygian Venus, ca. 200 AD. Over the millennia and across cultures, there has been an appreciation for a curvaceous, proportional gluteal region. The contour of the buttocks is defined mainly by the gluteus maximus muscle, and its augmentation is one of the fastest growing, most often requested procedures in plastic surgery today. This increased demand is in response to the growing desire of women to have buttocks that are larger, more rounded, and natural in contour. Surgery for buttock augmentation with implants began in 1969 when Bartels and colleagues performed a gluteal reconstruction using breast implants. During the 1970s, González-Ulloa was responsible for the development of specific implants for the gluteal region; however, a subcutaneous technique was used that proved inadequate as a result of a lack of support of the implants, which led to ptosis and capsular contracture. The submuscular technique, published in 1984 by Robles et al, provided good support to the prosthesis, with low rates of capsular contracture. However, implant positioning was limited to the cranial portion of the buttocks to avoid compression of the sciatic nerve, causing unaesthetic and unnatural results. The major technical progress occurred with the 1996 publication of an intramuscular technique by Vergara, because the implant, when positioned within the gluteus maximus muscle, has good support, low rates of capsular contracture, and better cosmetic results. Buttock augmentation can be performed using autologous tissue (fat grafts and flaps), silicone implants, or a combination of both techniques. Gluteal implants provide buttock reshaping and augmentation that is not always obtainable by other methods. The predictability of the results and small variation in volume lead to greater patient satisfaction than can be achieved through fat grafting alone. The intramuscular dissection is performed in the absence of a true anatomic plane. This is different from dissections for augmentation of the breast, pectoralis, or calf, where there is an anatomic plane to be dissected. It took extensive dissection of cadavers and surgical simulations to define the anatomic basis of the buttock augmentation technique. Fig. 18-2 The gluteus maximus is the thickest muscle of the human body, ranging from 4 to 7 cm thick. Patients who request augmentation of their buttocks often have a muscle thickness closer to 4 cm, which led us to define an optimal plan of dissection between 2 and 2.5 cm deep, in the middle of the gluteus maximus. There are major anatomic structures below the gluteus maximus muscle, including the superior and inferior gluteal arteries, which are responsible for muscle vascula-ture, the inferior gluteal nerve, and the sciatic nerve. Nerve branches and larger vessels (greater than 0.3 mm) are found in the deepest portion of the gluteus maximus, making dissection to 2 cm deep safe without creating physiologic changes. The intramuscular dissection does not make any changes in important anatomic structures, such as nerves and vessels, once these structures are in the submuscular space. The gluteus maximus muscle originates in the iliac crest, sacrum, coccyx, and sacrum tuberal ligament, and its insertion is into the fascia lata and femur bone. Its fibers run obliquely and inferiorly, offering a broad path for dissection and implant positioning. Anatomic Danger Zones ■ The superficial dissection and implant displacement occur more frequently at the superolateral gluteal zone. This is important, because the muscle is thinner and has a free edge at the point between the iliac crest origin and the fascia lata insertion. ■ A key to avoiding complications is to provide a wide base to the midline dermal fat island. The vessels in this area come from the bottom, so it is vital to preserve this area to have good blood supply and wound healing. The muscle atrophy is not clinically noticeable. The muscle function was studied through an isokinetic test, and there is no difference in the muscle function when compared with people who do not have buttock implants. The best candidates for augmentation gluteoplasty with implants are young women with a lack of volume or lack of projection in the gluteal region. Patients with true gluteal ptosis or senile buttocks are not good candidates for augmentation surgery alone; these patients should undergo gluteal lifting. Fig. 18-4 Gluteal implants are made of silicone gel or elastomer. The gel is cohesive and the covering is smooth. The implant shape may be round or oval. The oval one can be high or low profile. Patients with muscular hypotrophy of the gluteal muscles have often tried to increase muscle mass through physical activities without success, before looking for a plastic surgeon. The gluteal region becomes more flaccid and less bulky with age, weight variation, and pregnancies. The connections between the dermis and the fibrous gluteus fascia make this region more prone to lipodystrophy over time, with worsening of the sagging tissue. We often find patients with flabby buttocks and tissue accumulation in the lower third of the buttocks. Augmentation surgery can solve these kinds of issues. Patients who have too much skin laxity, such as postbariatric laxity, may need a gluteal lift in association with implants to improve this area. Oval implants should always be used in the oblique position, following the direction of the muscle fibers. Three months after the surgery, all oval implants will be in an oblique orientation because of the dynamics of the muscle. When examining a patient’s gluteal region, it is important to consider the relationship between the waist and hips, not just the buttocks in isolation. Some patients who are candidates for a gluteal implant procedure have a long body and a gluteus that is more vertical than wide. In such individuals the surgeon must use an implant that mimics the shape of the buttocks, such as an implant with an oval base. A round implant is indicated in patients with a short body, in whom the gluteal length and width are similar. The relationship between the waist and hip measurements is an important factor in what is considered the attractiveness of the female body, and ideally the ratio should be between 0.7:1 and 0.8:1. Patients whose ratio is above 0.9:1 will benefit from a combination of liposuction of the flanks and the use of low-profile implants. Because these patients have a wider gluteal base, the added liposuction will improve this relationship. The operation is performed under spinal or general anesthesia.
Buttock Augmentation With Implants
 Fernando Serra
Fernando Serra

Surgical Anatomy
Physiologic Considerations
Indications and Contraindications
IMPLANTS

Patient Evaluation
CLINICAL EVALUATION OF THE DEFORMITY
Preoperative Planning and Preparation
Surgical Technique
ANESTHESIA
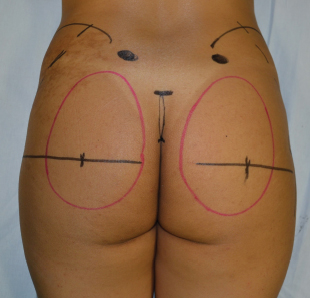
MARKINGS
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine