59. Buttock Augmentation
Sammy Sinno, Constantino G. Mendieta
BACKGROUND1
■ Buttock augmentation rapidly increasing in popularity
• 58% increase in 2014 in the United States according to the American Society for Aesthetic Plastic Surgery
• Over 35,000 patients have had gluteal implants placed in the United States and Brazil.
• Approximately 10,000 patients per year undergo buttock augmentation with fat grafting in the U.S.
• Celebrity and social media attention to gluteal augmentation has attracted even more interest in the general population.
■ Three major methods of augmentation
• Autologous fat grafting
• Silicone implants
• Autologous flap augmentation (in massive-weight-loss patients)
INDICATIONS2–4
■ Ideal for patients in good health who desire improved gluteal shape and contour
■ Thin patients typically have very dramatic results.
■ Overweight patients require additional liposuction to improve contour.
■ Slightly overweight patients are excellent candidates for autologous fat grafting.
• Excellent results seen for patients with excess sacral, lower back, and posterior triangle fat
SENIOR AUTHOR TIP: The choice of operation, autologous fat grafting versus silicone implants for gluteal augmentation is typically based on amount of fat available. If the patient has enough fat, a fat grafting is performed. If not, a gluteal implant is performed. To date, no systematic reviews exist that compare overall safety and efficacy of these two strategies (particularly for implants).
CONTRAINDICATIONS
■ Pregnancy
■ Neoplasm
PREOPERATIVE EVALUATION
■ Understand the anatomy of the gluteus maximus muscle (Fig. 59-1).
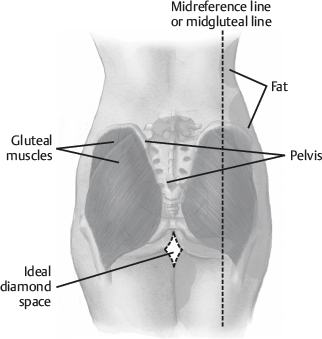
Fig. 59-1 Gluteus maximus muscle anatomy.
• Origin along lateral sacrum and continues upward to posterior iliac spine
• Attaches to superior iliac crest
• Inserts into iliotibial tract and greater trochanter
■ Divide each buttock into four quadrants.
TIP: Ideally, each quadrant should have equal volume.
■ Understand key anatomic landmarks (discussed below).
TIP: The lower inner gluteal fold ideally is diamond shaped.
■ Evaluate the buttock laterally.
• Presacral area should have a lazy-S shape.
■ Preoperative pinch test to evaluate donor fat areas
SENIOR AUTHOR TIP: For autologous fat grafting, ensure patients have enough donor fat, because the amount of fat needed can range from 450-1800 cc or greater per side.
INFORMED CONSENT
■ Fat grafting patients should be informed that lipoharvest, not liposuction, for removal is goal.
■ Silicone implant patients should be informed of risk of wound dehiscence, implant exposure, capsular contracture, infection, seroma, extrusion, and displacement.
■ Patients should be encouraged to avoid any medications that may promote bleeding before surgery.
■ Enema is given day before surgery.
■ Preoperative antibiotics are commonly given.
SENIOR AUTHOR TIP: Keep in mind that aesthetic ideals for gluteal augmentation may vary between ethnic groups.
EQUIPMENT
AUTOLOGOUS FAT GRAFTING2,5
■ Large-bore cannula (4 mm and 5 mm)
■ Several techniques for processing, including centrifugation, can be used but are time consuming.
TIP: A metal strainer can be used to irrigate and purify autologous fat.
■ Large-volume syringes (60 cc), Autoinfusion systems do not exist.
SILICONE IMPLANTS
■ Lighted retractors
■ Long instruments
■ Implant selection (silicone)
• High cohesive gel-filled texturized
• High cohesive gel-filled polyurethane surface cover
• Elastomer solid implant
• Can be anatomic, oval, or round shaped
TECHNIQUE
AUTOLOGOUS FAT GRAFTING (MENDIETA)6–10
■ Conceptualizing the 10 aesthetic units of the posterior region is essential.
■ Respecting these aesthetic units is crucial to obtain a smooth contour (Fig. 59-2).
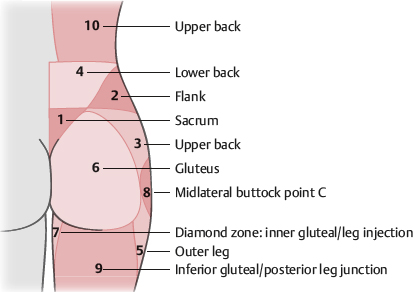
Fig. 59-2 Mendieta’s 10 aesthetic units or zones. (1, Sacrum; 2, flank; 3, upper back; 4, lower back; 5, outer leg; 6, gluteus; 7, diamond zone: inner gluteal/leg injection; 8, midlateral buttock point C; 9, inferior gluteal/posterior leg junction; 10, upper back.)
■ General or IV sedation
■ Patient marked standing; all zones
■ Landmark areas identified
• Posterior superior iliac spine (marks gluteal muscle height)
• Presacral “V” (superior point of intergluteal fold and posterior iliac dimples)
► Zone 1
► When liposuctioned creates desirable contour
• Midlateral buttock contour
► Ideally has no depression
■ Can give preoperative steroids for swelling, antibiotics, antireflux medications (patient will be in prone position)
■ Wetting solution injected
■ Supine position
■ Fat harvest through 5 mm cannula in deep layers and 4 mm cannula in superficial layers
• Most fat in buttock removed from zones 1, 2, 3, and 4
TIP: Typically, liposculpt zones 1 through 4, carefully liposuction in zone 5, and remember that fat transfer is difficult in zone 8 because of the paucity of muscle.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


