Chapter 17 Breast Reduction
Summary
Introduction
History of development of different techniques
In the 1970s McKissock1 introduced the vertical bipedicle breast reduction technique, which was the first procedure for breast reduction surgery that was both reliable and reproducible. Before then:
When it was discovered that either of McKissock’s pedicles could be severed, the inferior pedicle with an inverted T skin resection pattern became the favored method.6–8 It has a reliable blood supply to the nipple and areolar complex and the skin flaps close easily over the pedicle. The skin brassiere was tightened to control the breast shape. Although most surgeons around the world now use an inferior pedicle alone for the nipple and the Wise skin resection pattern9 for the skin, some still prefer the vertical bipedicle of McKissock, especially for larger reductions.
Meanwhile, the South Americans10–13 and the Europeans14–18 developed expertise with a vertical skin resection pattern and a vertical wedge resection of parenchyma. These techniques were used mainly for small reductions, with an inverted T skin resection pattern used for the larger reductions. Many of these surgeons used the superior pedicle19 for the nipple-areolar complex rather than the inferior pedicle, even when they chose an inverted T skin resection pattern. Many European and South American surgeons continue to use a superior pedicle, but often combine it with a Wise skin resection pattern.
Principles behind the techniques
The three main problems with breast reduction are:
Maintaining the blood supply
The breast is a superficial ectodermal structure that develops from the fourth interspace and its blood supply is superficial,20 except for the perforator through the pectoralis muscle. The perforator:
The superficial arteries comprise:
The veins do not accompany the arteries and are found separately (and seen) just beneath the dermis.
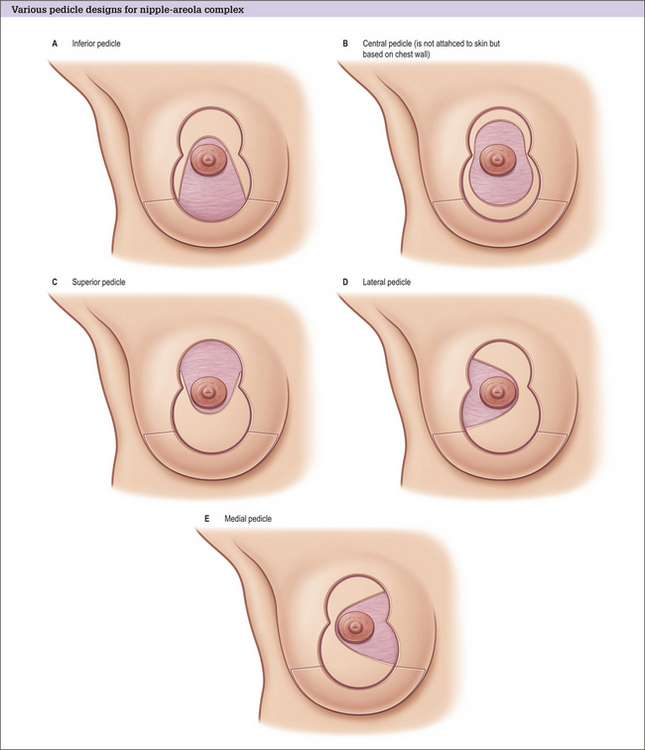
Types of pedicle
The blood supply of the different pedicles (Fig. 17.1A-E) is as follows:
Central pedicle
The central pedicle may not be quite as reliable as an inferior pedicle because there are many small but powerful blood vessels that enter the breast superficially from the level of the IMF. These are cut when a central pedicle is created. Creation of a central pedicle also severs the superficial veins, which supply most of the breast.
A central pedicle relies on the same arterial perforator and its venae comitantes as supply an inferior pedicle, and is therefore, by definition, full thickness.21,22
Free nipple grafts
Free nipple grafts are an important consideration especially if any of the other pedicles have an unpredictable blood supply,23,24 especially for the larger reductions. There is a loss of sensation, a loss of projection to the nipple, and a loss of breastfeeding potential. There is also a chance of irregular pigmentation.
Minimizing the risk of nipple necrosis
Although breast reduction is predictable and safe, there is a risk of complete nipple necrosis in around 1 in 300 patients. Some surgeons routinely use free nipple grafts, whereas many reserve these for the large reductions. The nipple is preserved with the Passot25 technique (or when a similar pedicle is used in a variation of the Robertson26 technique) where the complete inferior breast is used as a broad pedicle, and this is occasionally selected for extremely large reductions.
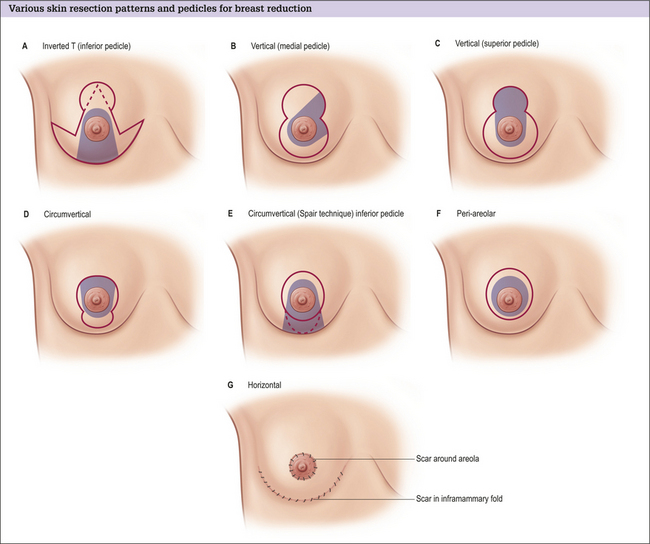
Skin resection pattern
The skin resection pattern (Fig. 17.2A-G) is determined mainly by the amount and quality of the excess skin.
Approaches to minimize scarring and maximize breast shape
The aim of further reducing scars is evident in the techniques that attempt to confine the scar to the area around the areola. The periareolar method is best suited for small breast reductions and some mastopexies.35,36 These are difficult procedures with a long learning curve. Separation of the skin flaps from the parenchyma is an essential component to achieve a good outcome.
Unanswered questions
Many questions are still debated by surgeons and include:
Indications
Choice of breast reduction operation
The most common skin resection patterns are the inverted T and the vertical techniques.
Inverted T resection
The inverted T resection is used for larger reductions and for patients with a large excess of skin, especially when there is poor skin elasticity (e.g. in patients who have had a massive weight loss).40
Vertical approach
The second most common skin resection pattern is the vertical approach. The most common pedicles are the superior and the medially based pedicles. Both the lateral and the inferior (short scar peri-areolar inferior pedicle reduction [SPAIR]30) pedicles are also used. Some surgeons take up more skin into the areola and call the procedure the ‘circumvertical’ approach.41,42 This is done to shorten the vertical scar, but does require more finesse in closing the areola without puckering and stretching.
Other techniques
Periareolar technique
For very small breast reductions, the periareolar technique can be used. This is a commonly misunderstood technique because it does not just involve suturing the skin under tension to the areola, but also involves separation of the skin from the breast tissue. The breast tissue is reduced and reformed35 with sutures or it is wrapped in various forms of mesh.36
For very large breast reductions, variations of the Passot25 technique can be used. In these cases, the pedicle is a complete inferior pedicle from medial to lateral. The upper skin flap is brought down over the inferior tissue and a cutout is then created for the areola. The upper skin flap is much longer than the incision along the IMF and a considerable amount of gathering is needed. This procedure is some-times called the ‘no vertical scar technique’ because the scar is confined to the IMF and the periareolar areas. Pribaz43 has modified the Robertson technique as a variation for the extremely large reductions. Rubin40 has developed a variation that can restore some shape for patients who have had massive weight loss.