CHAPTER 15 Breast Reduction with a Central Mound
Summary/Key Points
The use of an inferiorly based dermolipoglandular flap in reduction mammaplasty was first described in Brazil at the congress of the Brazilian Society of Plastic Surgery in 1971, and was first published in 1973.1 The flap has been mistakenly referred to as an ‘inferior pedicle.’
This inferior flap can also be used for the transposition of the nipple–areola complex in reduction mammaplasties and this possibility was introduced by the senior author in 1975,2 based on the follow-up of the patients operated upon this technique and analysis of the vascularization of this flap. This was later confirmed by the works of Robbins,3 and Courtiss and Goldwin,4 in 1977, who demonstrated that the principal sources of blood flow to the inferior pedicle are the perforating and intercostal branches of the internal mammary artery.
At present, the inferior flap is used in almost all mammaplasties performed in our practice, alone or in combination with another technique. We often use Peixoto’s principles,5 which result in reduction of the scars as in the lozenge technique.6–8
Anatomy
The inferiorly based flap is built from the inferior quadrants of the breast and has dermis, fat and mammary gland as its components. Its vascular supply is reliable and is made by branches of the internal mammary artery. It has an axial pattern with perforators of the intercostal vessels in greater number in the fourth, fifth and sixth intercostal spaces with an average diameter of approximately 1 mm (Fig. 15.1). These perforators are the main source of blood supply to the central and inferior segments of the breast. The venous drainage occurs in the opposite direction toward the internal mammary vein. The lymphatics drain to the internal mammary chain.

Indications and Patient Selection
The inferior flap technique with an inverted T skin resection pattern is indicated in cases of large breasts where the resection of tissue is expected to be over 500 g on each side, or in ptotic breasts where the skin is too flaccid. It is also indicated for less experienced surgeons in minor resections (see Figs 15.32 and 15.33). The lozenge technique cannot be used for every patient. The best results are attained in young patients with elastic skin and mild to moderate hypertrophy, even though we have made resections of up to 900 g on each side (see Fig. 15.34). Mild to moderate ptosis and as an adjunct in breast augmentation with correction of ptosis are also good indications.
I Inferior flap technique with inverted T skin resection pattern
Also called pedicle I (there are four more variants from the original flap numbered from II to V),7 it is used routinely in mammaplasties where the resection of tissue is expected to be over 500 g on each side, or in ptotic breasts were the skin is too flaccid. It is used with the skin markings of the Pitanguy technique,9 resulting in a breast with an ‘inverted T’ scar. The great advantage is the achievement of a conical and firm breast with long lasting result.
Operative technique (inverted T)
With the patient in a half-sitting position, the new areolae are drawn 4 cm in diameter with an areolar marker (Figs 15.2A and 15.3). A vertical line is drawn from the midclavicular line to the upper edge of the areolae, and point A is marked corresponding to the projection of the inframammary fold on the upper pole of the breast (Figs 15.2B and 15.4). By means of a pinching maneuver and the surgeon’s judgment, points B and C are marked, determining the amount of skin to be resected horizontally (Figs 15.2C and 15.5). The points are linked to the inframammary fold with curving lines, as in Pitanguy’s technique (Figs 15.2D, E, 15.6 and 15.7).
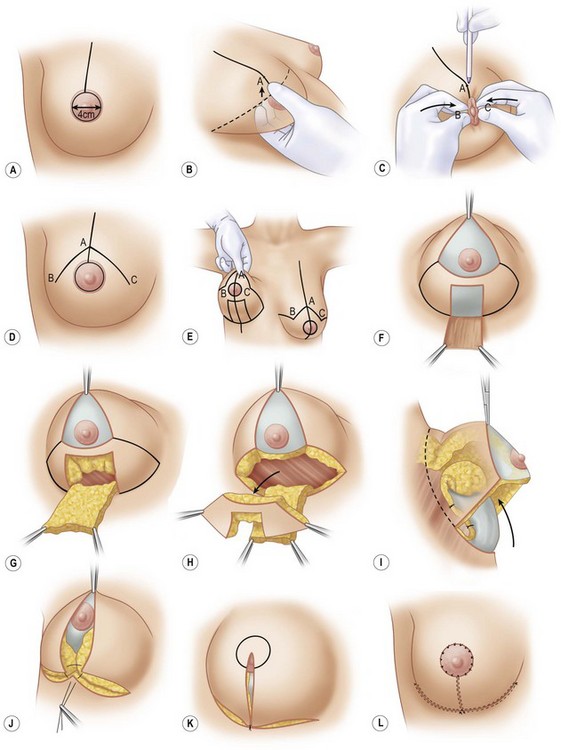





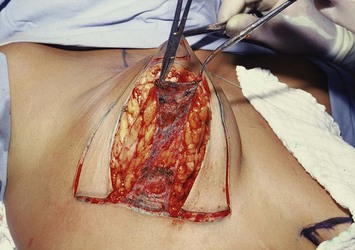
With the breast lifted so that the lower pole can be seen, the drawing of the flap is started at the central portion beginning in the inframammary sulcus and extending to 1 to 2 cm below the inferior edge of the areola. Its width is approximately 4 to 5 cm (Figs 15.2E and 15.7). The outlined flap is de-epithelialized (Fig. 15.2F), and an incision is made on its edges downward to the muscular plane to allow the shaping of a dermolipoglandular flap, supplied by the fourth, fifth, and sixth intercostal perforating vessels. It is important that the flap be 2 to 3 cm thick (Figs 15.2G and 15.8).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


