Chapter 16 Breast Augmentation
summary
To achieve successful breast augmentation results, it is crucial to:
Introduction
The female breast is a universal symbol of sexuality, motherhood and femininity today, dating back even to the time of ancient cave paintings. In the 1940s Alfred Kinsey observed that the female breast could inspire more sexual arousal in men than the sex organ.1 Since its introduction in 1962, modern breast augmentation with implants has become one of the most common aesthetic procedures, receiving more media attention than any other. However, much reporting, especially in the non-professional literature, has been faulty. More than one million breast implants are now inserted every year, 250 000 in the US. Most patients are very satisfied with the results.2 Most experience better psychological functioning and body image; many experience less anxiety and depression3 and even have better sexual relations with their partners. However, most women do not seriously contemplate the possibility of unfavourable results.4 Various complications are possible and should be seriously considered before undergoing a procedure. The risk should be minimized by a meticulous preoperative evaluation and surgical procedure. Selecting the ideal dimensions for implants, based on biological prerequisites, is crucial.
Patient and Implant Selection, Indications and Contraindications
Contraindications
The main contraindications are psychological. Patients must have realistic expectations of the procedure and understand benefits and risks. Those who do not understand, or are psychiatrically unstable and have unrealistic expectations are contraindicated. Clearly, a medical history and physical examination have to be undertaken to rule out health problems that may be contraindications. Older patients and patients with a genetic disposition for breast cancer should undergo a preoperative mammogram. General medical conditions such as diabetes mellitus and heavy smoking are only relative contraindications. Radiation therapy is a relative contraindication as it significantly increases the rate of capsular contraction.
Patient and Implant Selection
Patient communication
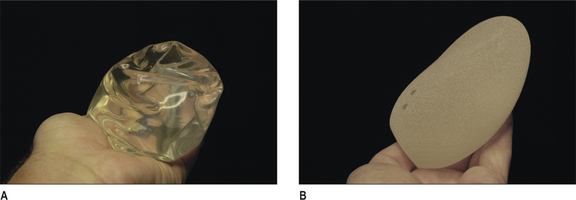
Previously, decision-making has been relatively arbitrary and based mainly on the surgeon’s experience without detailed measurements and analysis. In the last decade this has changed dramatically. Today, breast augmentation is no longer a ‘volumetric’ procedure, but a dimensional planning process. With the introduction of form-stable, high-cohesive silicone gel implants, dimensional planning has become crucial (Fig.16.1B). A low cohesive or liquid implant filler (Fig. 16.1A) can be deformed and made to fit in a poorly planned implant pocket, but with form-stable devices this is no longer the case.
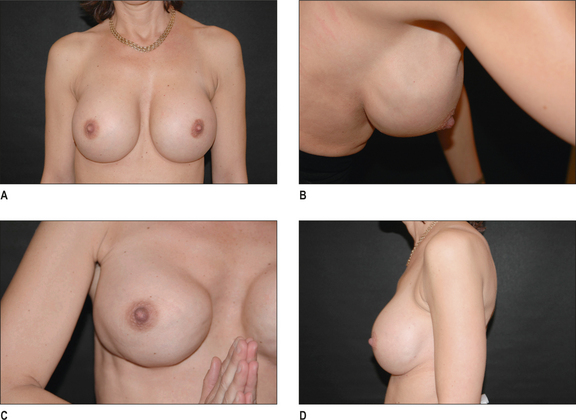
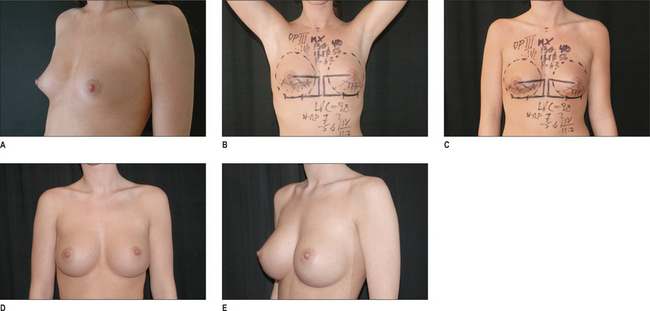
The first step in implant selection is the understanding of the patients’ expectations and desires. They must be told what the tissue limitations are and the drawbacks in selecting large implants should be clearly explained. During patient consultation, a full size mirror is useful to show the patient present and expected breast dimensions. Displacing the breast medial and lateral can easily demonstrate width limitations and the projection can be demonstrated with a calliper and by cupping the hand at the expected projection of the new breast. To use sizers in a tight-fitting sports bra may give the patient a certain feeling for the expected volume, but unless the patient is completely flat, this is of limited use in describing dimensions. The patient must understand that a condition for achieving the demonstrated breast dimensions is that no capsular contraction occurs in the postoperative phase (Fig. 16.2A-D). A severe capsular contraction could alter dimensions considerably, especially if low cohesive fillers are used (Fig. 16.3A-C & Fig. 16.4A & B).
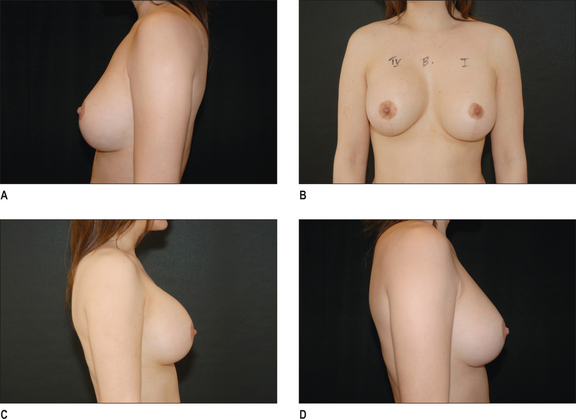
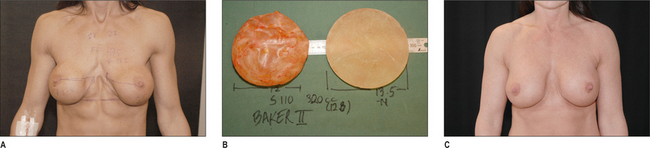
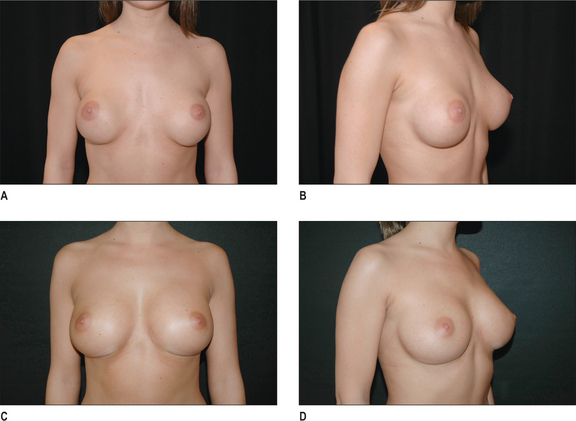
Fig. 16.3 A, After subglandular implantation in thin patients breasts have an unnatural appearance compared to sub-muscular implantation. B, Illustrates the implant with capsule on the left side and without on the right side. Only limited degree of capsular activity is noted in spite of the unnatural appearance in Figure 16.3A. C, After exchanging to implants in a new submuscular pocket.
Selection of implant filler, shape and surface
Only silicone gel and saline have been used long term and can be regarded as safe and proven. All implants consist of a solid silicone envelope. The surface may be textured or smooth. In the sub-glandular position, textured implants are favoured, whereas with sub-muscular placement, implants can be either smooth or textured (Fig. 16.1A & B). The benefit of silicone as a filling material is its softer, more ‘natural’ consistency and form (Fig. 16.5A-D). Saline implants have a higher rupture-risk, especially if these are not overfilled. However, the latter increases breast firmness. Silicone gel is available in a form-stable version; the round implant will retain its shape in standing position, as opposed to saline or standard responsive silicone gel implants, which become more position dependent. An anatomical high cohesive form-stable silicone implant will also maintain its anatomical shape in all positions. Form-stable silicone implants have a very low incidence of rupture.5
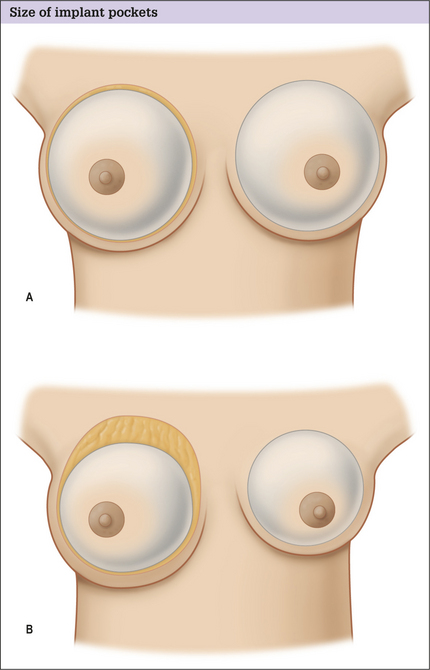
Selections of implant dimensions
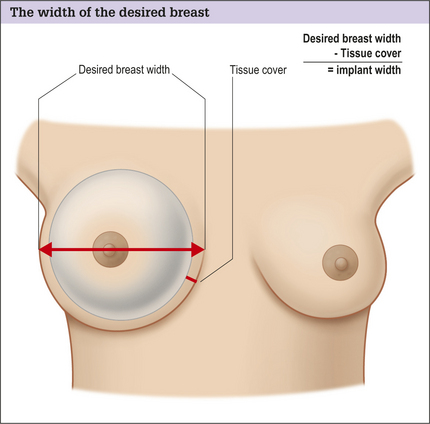
Regardless of implant type, a dimensional analysis should be undertaken. If high cohesive form-stable devices are used this is crucial, as these implants cannot be deformed. The most important dimension to define is the ideal implant-base width, which should be measured with a calliper. Existing glandular tissue width should also be measured. If an implant with a base width exceeding the existing breast width is selected, the risk of implant edge palpability and visibility is increased (Fig. 16.6A-D). However, with a very narrow breast base width, like that in tuberous and contracted breasts, the existing width must be exceeded for a natural appearance. The new desired inter-mammary distance is usually about 2-3 cm and laterally the anterior axillary line should be respected. Measuring the ideal width of the desired new breast provides information on ideal implant width if the tissue-cover is subtracted (Fig. 16.7). The covering tissue should be measured with a pinch-test at the expected inner border and at the lateral border of the new breast. These measurements should then be added together and divided by two, as a pinch is a double-fold of tissue. Subtracting the tissue cover from the ideal breast width provides the ideal implant width. From the implant manufacturers’ charts the implant dimensions are found and the upper border of the implant can also be calculated. This is done by elevating the arms 45 ° above the horizontal plane, simulating the expected, ideal nipple position after a correctly performed augmentation (Fig. 16.8A-D). This maneuver can be used to estimate where the upper border of the new implant will be, as half should be located above the nipple areola complex. This can be a useful guide in selecting the ideal implant shape and estimating the upper pole appearance of the augmented breast. When selecting implant projection, this is highly related to the tissue characteristics and to the patient’s desires. The selected projection together with the base dimensions of the implant supplies the implant volume. Implants are thus selected as a result of the dimensions of the ideal new breast and implant.
Preoperative history and psychological considerations
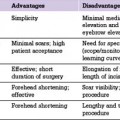
Patients who are unsuitable for surgery must be identified preoperatively. Andersson has proposed a number of questions that, if answered positively, should result in a further appointment before surgery as outlined in Table 16.1.6 During the evaluation, it must be stressed that breast augmentation complexity varies greatly. Tuberous breasts, severe ptosis, secondary augmentation cases and pronounced asymmetries are more difficult to correct.
Table 16.1 List of questions that, if answered affirmatively, warrants additional patient assessment