78
Brachydactyly
Scott H. Kozin
History and Clinical Presentation
A 5-year-old girl presented with a small right hand, mild webbing of the fingers, and an ipsilateral chest wall deformity. She is a product of a full-term, spontaneous, vaginal delivery. There were no problems during the pregnancy or at the time of delivery. She is otherwise healthy and has obtained normal developmental milestones (e.g., sitting, walking, and talking) at the appropriate time. There is no family history of similar deformities, including three siblings.
Physical Examination
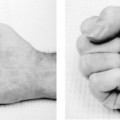
The patient is a healthy-appearing female with normal appearance and stature. The right chest wall appeared sunken with absence of the sternocostal portion of the pectoralis major muscle. Shoulder, elbow, and wrist had full motion and strength. The right hand was slightly smaller than the left, with mild webbing of the second (index-long) and third (long-ring) web space (Fig. 78–1). She had full dexterity of her digits and was able to form a full fist and claw.
Diagnostic Studies
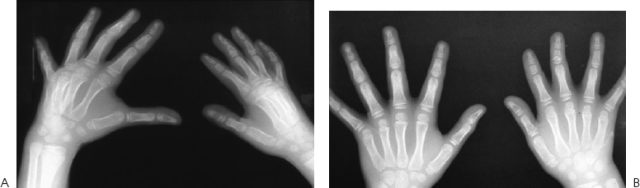
Radiographs of the chest and shoulder were normal. Several views of the hands revealed mild webbing of the second and third web spaces and shortened digits on the right hand, primarily at the middle phalangeal level (Fig. 78–2).
PEARLS
- All children with a hypoplastic hand should have their chest wall examined.
- Brachydactyly combined with syndactyly is often associated with Poland’s syndrome.
- Brachydactyly is most common at the middle phalanx level.
- Mild brachydactyly usually does not interfere with function.
PITFALLS
- Avoid surgery on mild brachydactyly.
- Avoid distraction osteogenesis at the phalangeal level in brachydactyly.
Differential Diagnosis
Brachydactyly associated with Poland’s syndrome
Clinodactyly
Camptodactyly
Pseudohypoparathyroidism
Pseudopseudohypoparathyroidism

Figure 78–1 A 5-year-old child with small right hand and mild syndactyly of the second and third web spaces.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


