This article reviews the current literature supporting the use of botulinum toxin in producing symmetric facial features and reducing unwanted, involuntary movements. Methods, protocols, and adverse events are discussed. Additionally, the authors suggest that using botulinum toxin A therapy in postparalytic facial synkinesis can provide long-term results when used in conjunction with other treatment modalities.
Key points
- •
Combination treatment with neuromuscular retraining (NMR) exercises is essential for a better long-term outcome.
- •
A sequence of first evaluation and treatment with NMR is recommended. When resistant muscle groups are identified, treatment should be started with chemodenervation.
- •
Botulinum toxin can be injected in the affected synkinetic hemiface to relax hyperactive muscles and the normal hemiface for balance to restore facial symmetry.
- •
Challenging areas for treatment of synkinesis include the midface and lip depressor complex and should be addressed carefully.
Introduction
Synkinesis makes up the overwhelming majority of patients who present to a facial nerve center with facial movement disorders. The synkinetic facial movement can be subtle or completely disfiguring. Interestingly, patients who have synkinetic activity that is barely noticeable sometimes are the most disturbed by the condition. Most patients begin to see evidence of spastic activity of the facial muscles 6 months after recovery of their facial paralysis. Rarely, this can even occur in the early phase of recovery as well. Synkinetic activity should only occur on the hemifacial side of the original injury.
Restoration of permanent facial symmetry in the postparalyzed synkinetic face has been a mainstay of surgical treatment. Myectomy, neurectomy, cross-face nerve grafts, and sling procedures have all been implemented in achieving outcomes. Although results can be satisfactory, they are invasive and irreversible. Botulinum toxin with and without neuromuscular therapy has shown promising utility as a nonoperative method in restoring normal facial features, with recent literature demonstrating increasingly long-term effects when used concurrently with neuromuscular training.
Produced by various strains of Clostridium botulinum , multiple agents are currently available on the United States market. There are currently 4 pharmacologic forms in the United States, each with varying potencies and shelf lives: abobotulinumtoxinA (Dysport, Medicis Aesthetics, Inc, Scottsdale, AZ; Azzalure, Galderma Laboratories, Lausanne, Switzerland), incobotulinumtoxinA (Xeomin, Merz Aesthetics, Inc, Franksville, WI), onabotulinumtoxinA (Botox, Allergan, Inc, Irvine, C), and rimabotulinumtoxinB (Myobloc, Solstice Neurosciences, LLC, Louisville, KY). Application remains percutaneous and intramuscular. Pattern of injection into muscle groups, units administered, and frequency of treatment is not standardized. Amounts administered have varied from fractions of a unit per site to hundreds in total, with increasing risk of adverse events including oral incompetence, ptosis, diplopia, exposure keratopathy, malaise, and worsened cosmesis with larger doses. These events are reversible, however, because the effects of the toxin diminish.
Botulinum toxin continues to expand from its first description in strabismus by Scott in 1980 to its eventual approval by the US Food and Drug Administration for strabismus and blepharospasm in 1989. Additional benefits were recognized for aesthetic purposes by Carruthers and Carruthers in their description of reduction in glabellar frown lines in 1992.
Those who endure the sequela of postparalytic synkinesis or abnormal involuntary facial movements have been shown to have diminished quality of life, social interactions, peripheral visual impairment, and a worsened self-impression of personal appearance. In many instances, botulinum toxin therapy has been shown to decrease the severity of these personal morbidities and improve quality of life with validated methods of subjective assessment including the Facial Clinimetric Evaluation score, Sunnybrook Facial Grading System, and Synkinesis Assessment Questionnaire currently in use.
Characterized by involuntary movement in the setting of volitional facial expressions, multiple patterns have been described after facial nerve injury including ocular, oral, and cervical synkinesias, dyskinesias, and hyperkesias. Typically, a patient might experience spasm of the eye with smiling or sometimes violent movements of the corner of the mouth with eye closure. Manifestations of various forms require personalized injection patterns to achieve optimal outcomes and aesthetics while minimizing side effects. The toxin is typically administered to certain muscle groups that provide certain function (ie, eye closure or lip elevation) such as injection into the orbicularis oculi, corrugators, and frontalis muscles for upper synkinesias and zygomaticus, levator muscle of upper lip, orbicularis oris, depressor labii, depressor oris, and platysma muscles for lower division defects. Functionally, botulinum toxin chemically dennervates the neuromuscular junction by permanently blocking presynaptic acetylcholine release at the synaptic junction.
Mention of botulinum toxin A as an alternate treatment of ocular synkinesia was first introduced by Putternam in 1990. In his description of a single case report, he discusses a 28-year-old woman with “misdirection of the facial nerve” after Bell’s Palsy causing ocular spasm with smiling. Since then, the literature has been populated by numerous studies augmenting the role of botulinum toxin A in postparalytic facial synkinesia evolving to hints of long-term improvement when used with concurrent neuromuscular training including half and whole face mirror feedback and neuromuscular retraining (NMR) therapy. The application of other traditional therapies in conjunction with botulinum toxin has yet to be elucidated.
Causes of postparalytic facial synkinesia are vast and varied, providing a universal platform for this minimally invasive therapy. Central iatrogenic tumor resections in the setting of vestibular and facial schwannomas, middle ear surgery, as well as peripheral parotid malignancies have been described. Bells palsy and Ramsey Hunt syndrome have also been implicated, in addition to traumatic skull base injury.
The neurophysiology of these involuntary movements has yet to be fully understood. Aberrant peripheral facial nerve regeneration is most commonly attributed. However, studies in the generation of synkinesis have demonstrated predictable patterns of regeneration thought to be owing to increased excitability within the facial nucleus itself.
This article reviews the current literature supporting the use of botulinum toxin in producing symmetric facial features and reducing unwanted, involuntary movements. Methods, protocols, and adverse events are discussed. Additionally, the authors suggest that using botulinum toxin A therapy in postparalytic facial synkinesis can provide long-term results when used in conjunction with other treatment modalities.
Introduction
Synkinesis makes up the overwhelming majority of patients who present to a facial nerve center with facial movement disorders. The synkinetic facial movement can be subtle or completely disfiguring. Interestingly, patients who have synkinetic activity that is barely noticeable sometimes are the most disturbed by the condition. Most patients begin to see evidence of spastic activity of the facial muscles 6 months after recovery of their facial paralysis. Rarely, this can even occur in the early phase of recovery as well. Synkinetic activity should only occur on the hemifacial side of the original injury.
Restoration of permanent facial symmetry in the postparalyzed synkinetic face has been a mainstay of surgical treatment. Myectomy, neurectomy, cross-face nerve grafts, and sling procedures have all been implemented in achieving outcomes. Although results can be satisfactory, they are invasive and irreversible. Botulinum toxin with and without neuromuscular therapy has shown promising utility as a nonoperative method in restoring normal facial features, with recent literature demonstrating increasingly long-term effects when used concurrently with neuromuscular training.
Produced by various strains of Clostridium botulinum , multiple agents are currently available on the United States market. There are currently 4 pharmacologic forms in the United States, each with varying potencies and shelf lives: abobotulinumtoxinA (Dysport, Medicis Aesthetics, Inc, Scottsdale, AZ; Azzalure, Galderma Laboratories, Lausanne, Switzerland), incobotulinumtoxinA (Xeomin, Merz Aesthetics, Inc, Franksville, WI), onabotulinumtoxinA (Botox, Allergan, Inc, Irvine, C), and rimabotulinumtoxinB (Myobloc, Solstice Neurosciences, LLC, Louisville, KY). Application remains percutaneous and intramuscular. Pattern of injection into muscle groups, units administered, and frequency of treatment is not standardized. Amounts administered have varied from fractions of a unit per site to hundreds in total, with increasing risk of adverse events including oral incompetence, ptosis, diplopia, exposure keratopathy, malaise, and worsened cosmesis with larger doses. These events are reversible, however, because the effects of the toxin diminish.
Botulinum toxin continues to expand from its first description in strabismus by Scott in 1980 to its eventual approval by the US Food and Drug Administration for strabismus and blepharospasm in 1989. Additional benefits were recognized for aesthetic purposes by Carruthers and Carruthers in their description of reduction in glabellar frown lines in 1992.
Those who endure the sequela of postparalytic synkinesis or abnormal involuntary facial movements have been shown to have diminished quality of life, social interactions, peripheral visual impairment, and a worsened self-impression of personal appearance. In many instances, botulinum toxin therapy has been shown to decrease the severity of these personal morbidities and improve quality of life with validated methods of subjective assessment including the Facial Clinimetric Evaluation score, Sunnybrook Facial Grading System, and Synkinesis Assessment Questionnaire currently in use.
Characterized by involuntary movement in the setting of volitional facial expressions, multiple patterns have been described after facial nerve injury including ocular, oral, and cervical synkinesias, dyskinesias, and hyperkesias. Typically, a patient might experience spasm of the eye with smiling or sometimes violent movements of the corner of the mouth with eye closure. Manifestations of various forms require personalized injection patterns to achieve optimal outcomes and aesthetics while minimizing side effects. The toxin is typically administered to certain muscle groups that provide certain function (ie, eye closure or lip elevation) such as injection into the orbicularis oculi, corrugators, and frontalis muscles for upper synkinesias and zygomaticus, levator muscle of upper lip, orbicularis oris, depressor labii, depressor oris, and platysma muscles for lower division defects. Functionally, botulinum toxin chemically dennervates the neuromuscular junction by permanently blocking presynaptic acetylcholine release at the synaptic junction.
Mention of botulinum toxin A as an alternate treatment of ocular synkinesia was first introduced by Putternam in 1990. In his description of a single case report, he discusses a 28-year-old woman with “misdirection of the facial nerve” after Bell’s Palsy causing ocular spasm with smiling. Since then, the literature has been populated by numerous studies augmenting the role of botulinum toxin A in postparalytic facial synkinesia evolving to hints of long-term improvement when used with concurrent neuromuscular training including half and whole face mirror feedback and neuromuscular retraining (NMR) therapy. The application of other traditional therapies in conjunction with botulinum toxin has yet to be elucidated.
Causes of postparalytic facial synkinesia are vast and varied, providing a universal platform for this minimally invasive therapy. Central iatrogenic tumor resections in the setting of vestibular and facial schwannomas, middle ear surgery, as well as peripheral parotid malignancies have been described. Bells palsy and Ramsey Hunt syndrome have also been implicated, in addition to traumatic skull base injury.
The neurophysiology of these involuntary movements has yet to be fully understood. Aberrant peripheral facial nerve regeneration is most commonly attributed. However, studies in the generation of synkinesis have demonstrated predictable patterns of regeneration thought to be owing to increased excitability within the facial nucleus itself.
This article reviews the current literature supporting the use of botulinum toxin in producing symmetric facial features and reducing unwanted, involuntary movements. Methods, protocols, and adverse events are discussed. Additionally, the authors suggest that using botulinum toxin A therapy in postparalytic facial synkinesis can provide long-term results when used in conjunction with other treatment modalities.
Evaluation
Before beginning therapy, a patient should undergo a thorough evaluation of their history of facial paralysis and a complete evaluation of their facial movements. Standardized photography and video recording should be performed to clearly document treatment efficacy. The 9 standard views include face at rest, brow elevation, complete eye closure, nose wrinkling, grin, full smile, pucker, whistle, and lower lip depression.
It is important during the evaluation to identify the “triggers” for eliciting the synkinesis. This most commonly is forceful eye closure or a puckering movement of the lips. Critical to the evaluation, the patient should be questioned their main concerns are and what areas of the face and neck are the most troubling. Patients typically remark about the discomfort of spasms around the eye or neck. Ideally, these areas should be addressed first and foremost. It is recommended to wait at least 6 months after the onset of facial paralysis to allow recovery. Any intervention before that time can potentially make the synkinesis worse.
Ideally, the patient should have an initial treatment by a physical or occupational therapist who has specific training in facial NMR. It is helpful for the physician to evaluate the patient before beginning therapy, which can help to determine the progress of treatment. A team approach can be very helpful to the patient.
Therapeutic options
Neuromuscular Retraining
Facial NMR is a specific subset of occupational and physical therapy developed for improving motor learning and functional outcomes in patients with facial paralysis, paresis and/or synkinesis after facial nerve injury. Facial NMR techniques are based on characteristics unique to the facial nerve and muscles it innervates (eg, lack of muscle spindles and presence of emotional, as well as volitional, neural inputs). Facial NMR should not be confused with the more common, nonspecific therapies that promote gross motor, maximum effort exercises and electrical stimulation, both of which are contraindicated in facial paralysis. Rather, NMR focuses on providing sensory information to enhance neural adaptation and learning via the practice of minimal, precisely coordinated movement patterns in conjunction with modalities such as surface electromyographic, proprioceptive, and mirror feedback. This comprehensive clinical program was first described by Balliet and colleagues in 1982, who reported improved function in patients more than 2 years after facial nerve injury. Acquisition of new motor behaviors was attributed to brain plasticity, the capacity of the central nervous system to modify its organization, resulting in lasting functional change.
From a nonoperative rehabilitation perspective, facial muscles play a different role than other muscles in the body. Simply stated, their purpose is to move the facial skin in various directions, producing a wide variety of expressions used primarily for nonverbal communication, eye closure, and oral motor functions. The subtleties of human expression require a delicate balance of activity among multiple facial muscles. The presence of synkinesis destroys the normal balance.
Synkinesis is the most common condition treated by the facial NMR therapist. Because it does not occur in other areas of the body, there is no precedent for identifying and understanding it. When muscles contract out of sequence, the facial skin is displaced in an unusual direction, creating a distorted expression. What seems to be lack of movement caused by weakness may in fact be abnormal hyperactivity of an opposing muscle restricting range of motion and excursion.
Comprehensive retraining incorporates significant education regarding facial anatomy and muscle actions. This is key to comprehending the true nature of the disability, that is, the difference between a deficiency of muscle activity resulting in no movement (flaccidity) and aberrant muscle activity (synkinesis) resulting in wrong movement. In cases of synkinesis, the common practice of prescribing maximum effort movements (in an erroneous attempt to strengthen muscles) intensifies the abnormal response, reinforcing the synkinesis. Appropriate intervention focuses on accurately coordinating viable, albeit synkinetic, muscles rather than stimulating flaccid ones. With skilled training it is possible to improve movement patterns and expression even many years after synkinesis develops.
When used in conjunction with facial NMR, botulinum toxin provides a “window of opportunity” during which the patient can learn and practice isolated, coordinated movement patterns without the cocontraction and restriction caused by synkinesis. It is preferable to complete 6 months of retraining before injecting botulinum toxin to enable the patient to learn the synkinesis inhibition techniques. The presence of botulinum toxin before retraining does not afford this same learning opportunity.
The retraining therapist, as part of the multidisciplinary team, is instrumental in precisely identifying the synkinetic muscles most restricting normal function. These, when injected, should allow for greater ease and range of motion in keeping with the patient’s stated goals, without causing additional morbidity. Targeting the most appropriate injections sites for the best outcome is challenging owing to the complex interactions of the facial muscles. Knowledge of anatomy is not enough. It is also essential to know the working action of each muscle, both in isolation and in conjunction with the actions of others.
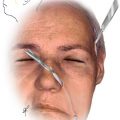
The most common injection sites include the orbicularis oculi, corrugator, platysma, and mentalis muscles ( Fig. 1 ). Recently, minimal dose injections to the synkinetic buccinator have proven to be of benefit in improving outcomes. The midfacial muscles are rarely injected to avoid creating weakness in key areas targeted during the NMR process, such as smile. For greatest accuracy in targeting injection sites, the patient is asked to demonstrate the expressions that elicit the synkinetic response. Forceful eye closure, smile, pucker and snarl will most commonly produce the response. Each movement may elicit a unique synkinetic pattern, so all should be tested. It is important to note that even a region demonstrating little to no volitional activity (e.g. forehead) can demonstrate significant aberrant activity in a synkinetic pattern, so should be evaluated in that context. (In such a case, no brow movement is observed when the patient attempts to raise it volitionally, however, significant elevation may occur during smile or pucker).