Successful weight loss is achieved through bariatric surgery and medications like Tirzepatide and Semaglutide. However, this often results in significant loose skin. Developing a personalized surgical plan for body contouring to address the loose skin can have a transformative impact on a patient’s quality of life.
Key points
- •
Personalized Surgical Planning : Creating a custom plan to address loose skin after significant weight loss can greatly improve a patient’s quality of life.
- •
Preoperative Evaluation : Assess the patient’s health, expectations, goals, and optimal surgery timing, while planning procedures based on patient needs and recovery capacity.
- •
Treatment Areas : Body contouring targets areas like the arms, abdomen, breasts, and thighs, which can be treated together or staged based on surgery time.
- •
Recovery Preparation : Patients should allow adequate recovery time, including time off work, to ensure optimal results and reduce the risk of complications.
Introduction
More patients are achieving successful weight loss thanks to bariatric surgery and medications like Tirzepatide and Semaglutide. However, this often results in significant loose skin. Developing a plan to address this can seem daunting, but by discussing the patient’s goals, evaluating medical conditions that may impact healing, and educating them on available procedures, you can create a personalized surgical plan to meet their needs.
Preoperative Evaluation
Medical and pre-operative considerations
Before undergoing body contouring procedures, patients should be in overall good health. Significant contraindications include known cardiac disease such as uncontrolled hypertension, arrhythmias, or the presence of pacemakers/defibrillators, as well as uncontrolled diabetes, typically indicated by an HbA1C greater than 7%. Nicotine use, whether from smoking or vaping, is another contraindication due to its negative impact on wound healing and increased risk of infection. Patients who smoke or vape should be advised to stop for at least 4 weeks prior to surgery, as well as for 4 to 6 weeks after surgery. Compliance can be verified with a urine cotinine test.
Additionally, patients should be at a stable weight for at least 3 months. This ensures that they are not continuing to lose weight, which could impact the results of body contouring procedures. Rather than relying on strict body mass index thresholds, the decision to proceed with surgery should be based on a realistic assessment of the patient’s ability to maintain long-term weight loss. During the physical examination, specific areas of fat distribution should be evaluated, as each patient’s body stores fat differently. Even if a patient is not at their ultimate goal weight, certain areas may show minimal fat, such as the upper arms, which might not benefit much from additional weight loss.
Patients who have gone through bariatric surgery are at risk for protein deficiency— Protein deficiency (serum albumin <3.5 mg/dL) remains the most severe macronutrient complication associated with malabsorptive surgical procedures [ ]. Post-bariatric surgery patients are advised to take in 60g to 80g per day of protein, or 1g/kg to 1.5 g/kg of ideal body weight to support wound healing. This same recommendation applies to patients on medications like Semaglutide and Tirzepatide, which suppress appetite and can make it harder for patients to meet their nutritional needs. Protein supplements, such as whey protein, may also be helpful.
A discussion of the pre-operative evaluation would not be complete without a discussion of deep vein thrombosis (DVT) risk and prevention. Patients are typically assessed for their risk of DVT using the Caprini score during the preoperative visit. All patients with a Caprini score of 7 or higher are given subcutaneous enoxaparin starting on the first postoperative day [ ].
Surgical planning and procedure selection
When considering body contouring procedures, it is important to assess the patient’s specific concerns and priorities. In our experience, the most common areas for skin removal include the upper arms (brachioplasty), breasts (mastopexy, augmentation, or reduction), abdomen (abdominoplasty), and thighs (thigh lift). While many patients do not specifically request a posterior body lift, it is essential to evaluate the back and assess it as part of a comprehensive, circumferential approach. For optimal results, the back and trunk should often be addressed together, and it may be beneficial to stabilize the trunk with these procedures (abdominoplasty and posterior body lift) prior to proceeding with additional procedures since the abdomen and back will impact the breast and thighs. The patient’s goals should guide the procedure selection, but these and other anatomic considerations also play a role. For example, brachioplasty and mastopexy are often performed together due to their proximity.
In evaluating the patient’s body, both subcutaneous and visceral fat must be considered. Subcutaneous fat is assessed by skin pinch, while visceral fat can affect the results of abdominoplasty and is evaluated by having the patient relax and contract their abdominal muscles to assess the degree of abdominal prominence. Diastasis (separation of abdominal muscles) may also contribute to a prominent abdomen, and in cases where visceral fat is limiting results, patients with significant skin overhang may still benefit from improved body contouring assuming that appropriate expectations are set preoperatively. It is important to review preoperative photos with the patient to discuss what is realistically achievable and then set expectations accordingly.
Combining and staging procedures
When planning the sequence of procedures, it is crucial to balance the patient’s priorities with total operative time. The American Society of Plastic Surgeons recommends a maximum of 6 hours for surgeries performed in an ambulatory setting. While combinations of procedures that target anatomically close areas (such as brachioplasty with mastopexy) often make sense, the patient’s preferences and anatomic considerations should dictate the final plan. In some cases, it is beneficial to stabilize the trunk first before performing procedures on other body areas, such as the breast or thighs. A circumferential body lift or trunk stabilization may improve the overall outcome and serve as a foundation for addressing other areas later.
When discussing the timing of the staged procedures, patients should be advised to wait at least 3 to 6 months between stages to allow for proper recovery. This also provides an opportunity for revisions or touch-ups if needed. In some cases, staging can be based on anatomic proximity and patient preferences, with related surgeries being grouped together, while more distant procedures (eg, brachioplasty and thigh lift) can still be safely performed in a single operative session.
Surgical location—ambulatory surgery center versus inpatient hospitalization
In recent years, the majority of body contouring procedures are being performed in ambulatory surgery centers (ASCs) or office-based operating rooms, as opposed to inpatient settings. The safety of performing these procedures in an outpatient setting has been well-established, with studies showing similar outcomes to inpatient procedures. In fact, ASCs have several advantages: they provide a more intimate, patient-focused environment, reduce costs, and allow for quicker recovery due to the ability for early mobilization. While these procedures were once commonly performed in the hospital setting, ASCs have proven to be a safe and effective alternative that offers patients greater convenience and more personalized care. Procedures performed in an ASC are reserved for patients ASA III or less; therefore, patients with multiple medical comorbidities may benefit from a procedure performed in a hospital.
Surgical technique
Brachioplasty and Extended Brachioplasty
Brachioplasty removes the excess skin of the upper arm, sometimes extending the incision across the elbow to address the lower arm. Patients see an improvement in how clothing fits over the upper arm, especially with more form-fitting clothing such as blazers and may feel more comfortable in sleeveless clothing. The greatest downside to brachioplasty is the scarring, since the scars fade less than those from other skin-removal operations.
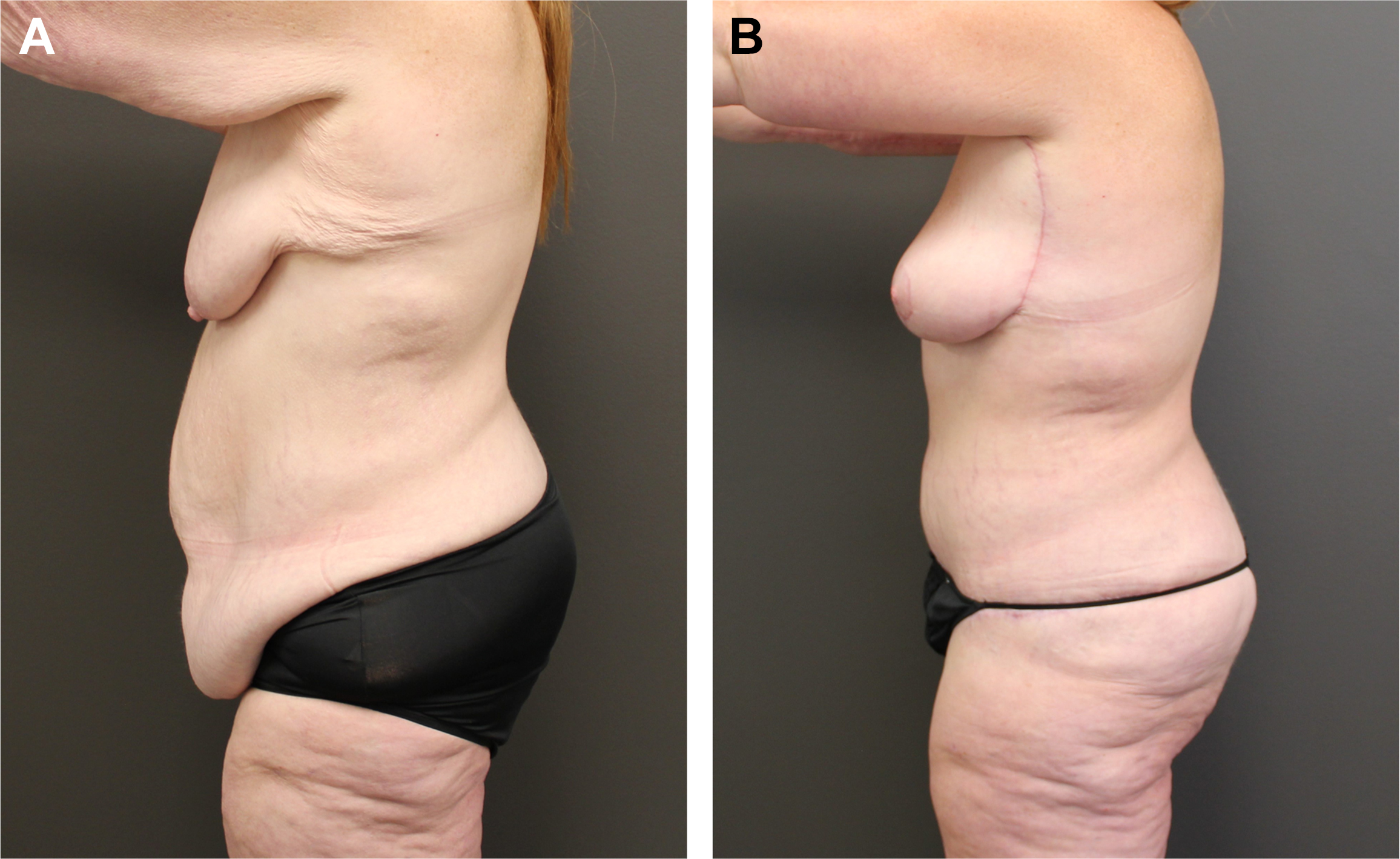
Traditional brachioplasty extends from the axilla to the elbow. The extended brachioplasty continues the incision inferiorly along the lateral chest, curving into the inframammary crease (Deborah White M.D., Deborah White M.D. Plastic Surgery, email, October 20, 2020). This extension removes excess skin over the lateral chest, which may spill over the bra or form a roll along the inframammary crease ( Fig. 1 A, B ).
Mini-brachioplasty uses an incision along the axillary crease to remove skin, but it is less effective for post-bariatric patients as it only targets the upper third of the arm. It is also prone to wound healing issues but can be a useful revision option for patients who have had a full brachioplasty and developed additional skin laxity over time.
Markings
Brachioplasty markings are made with the patient standing and arms outstretched at shoulder height. Initial markings are done with the elbow extended to relax the triceps, creating more laxity over the posterior arm. The incision is centered midway between the bicipital groove and the posterior arm to ensure the scar is hidden when the arm is relaxed. Areas of excess fat, often above the elbow, are marked for potential liposuction to improve contour. For extended brachioplasty, the markings extend down the lateral chest and curve into the inframammary fold. The axilla should not have significant skin removed to avoid webbing, and a Z-plasty is rarely needed if minimal skin is excised.
Positioning
The patient is positioned supine with the elbows extended and shoulders abducted at 90°, using regular arm boards. Intravenous access should be placed in the dorsum of the hand with a heplock attached. If an extended brachioplasty is being done, taping the breasts in a medial position will improve exposure. The arms are prepped circumferentially, and the hands can either be covered with stockinette or simply toweled off.
Skin excision is performed using the avulsion method described by Hunstad and colleagues [ ] A superwet rather than tumescent technique is used to limit the amount of wetting solution left after aspiration. Aspiration is performed aggressively under the planned area of skin excision with the purpose of debulking subcutaneous adipose tissue and dissecting out the deep plane. Once aspiration is complete, the skin is incised down to the level of aspiration and avulsed using a kocher clamp. Hemostasis is obtained with cautery. Closure is performed in layers with absorbable sutures.
Once skin closure is complete the incisions are dressed with a self-adhesive mesh combined with 2-octyl cyanoacrylate (Prineo). The patient is then placed in compression sleeves or a dressing with an ACE wrap.
Abdominoplasty
Abdominoplasty allows for repair of rectus diastasis and effectively removes excess skin over the lower abdomen. Many patients have excess skin superior to the umbilicus in both the horizontal and vertical dimensions. Fleur-de-lis (FDL) abdominoplasty removes this skin by adding a vertical incision as well, and should be a consideration in patients who have lost 50 pounds or more. Although the vertical scar is visible in a 2-piece bathing suit, scars in this location fade with time. The FDL abdominoplasty has the additional benefit of creating a neo-umbilicus [ ], which looks natural because the scar goes through, rather than around it.
Markings
Patients are marked for the abdominoplasty while standing. Skin is first retracted superiority to expose the mons pubis. The mons may become ptotic after pregnancy and weight loss, so upward traction on the area while marking is critical to correct the ptosis. The horizontal incision will fall within the hair-bearing skin, approximately 5 to 7 cm superior to the vulvar cleft. The incision curves gradually upwards on each side, crossing the anterior-superior iliac spine. The midline is marked from the xiphoid to the mons. For an FDL abdominoplasty, the vertical skin excision is initially marked with the patient standing, and then adjusted once on the operating room (OR) table.
Positioning
Abdominoplasty is performed with the patient supine—the bed should be checked to ensure that it flexes at the appropriate point. If the patient is placed in the lithotomy position for a concurrent thigh lift, one must be cognizant of the fact that the lithotomy position has risks related to prolonged positioning including neuropraxia, DVT, and strain on the hip joint. For this reason, it may be advisable to reposition and drape the patient after the abdominal surgery is completed, depending on planned total surgical time.
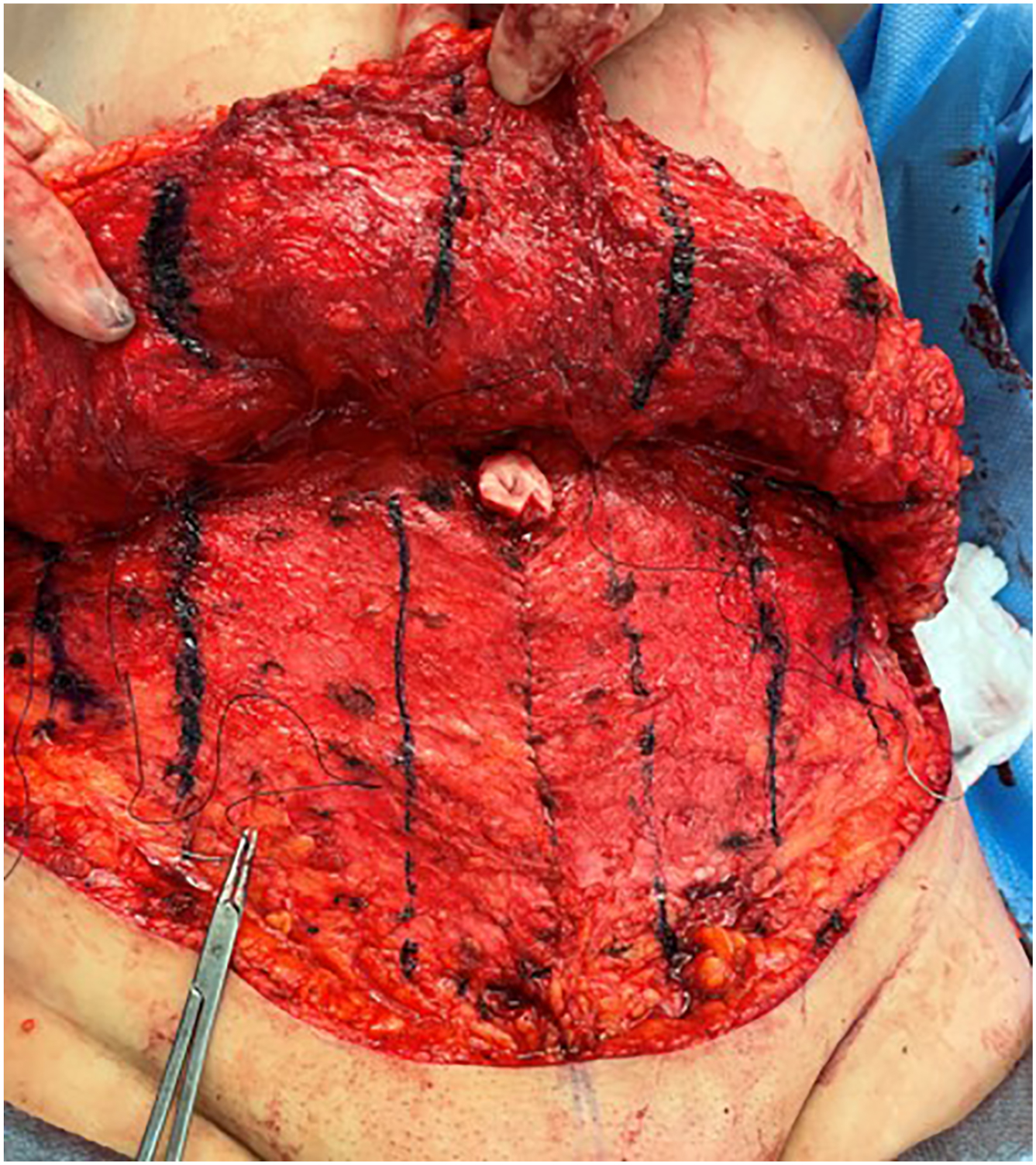
Because the lower abdominal incision is marked with upward tension on the skin to maintain a low position of the incision after closure, the lower aspect of the skin flap often overlays the inguinal lymph nodes. Placing vertical tension on the skin flap using Kochers will help maintain the correct plane of dissection and avoid damaging the lymphatics. After removal of the excess skin the rectus diastasis is repaired. Progressive tension sutures using 2-0 polydioxanone (PDS) in a barbed suture are placed between the Scarpa’s fascia and anterior rectus sheath to advance the skin flap and close dead space ( Fig. 2 ). Patients are then flexed at the waist to allow proper placement of the umbilicus. For the FDL abdominoplasty, the umbilical tabs are tacked to the anterior rectus sheath with three 3-0 nylon sutures ( Fig. 3 ). The Scarpa’s fascia is then closed with 2-0 PDS barbed sutures, and the skin with 4-0 monoderm barbed suture.