39. Blepharoptosis
Jason E. Leedy, Jordan P. Farkas
DEFINITION
Blepharoptosis is drooping of the upper lid margin to a position that is lower than normal. (Normal upper lid position is at the level of the upper limbus.)
ANATOMY1 (Fig. 39-1)
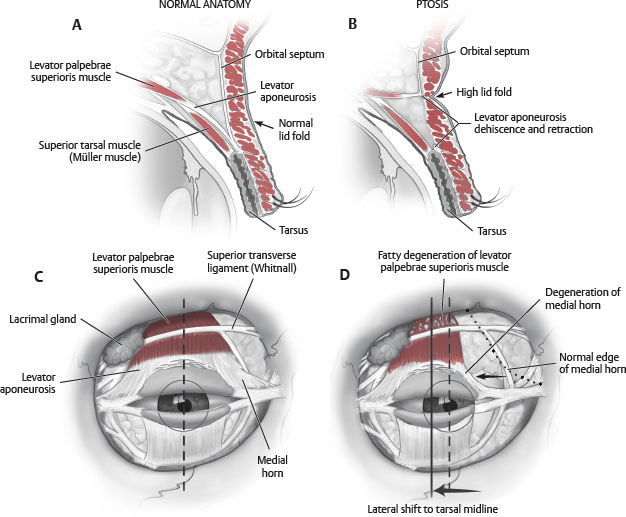
Fig. 39-1 Differences between normal and ptotic upper eyelid anatomy.
LEVATOR APONEUROSIS
■ Origin: Lesser wing of the sphenoid
■ Insertion: Orbicularis oculi, dermis, tarsus
■ Innervation: Superior division of oculomotor nerve (CN III)
■ Action: Provides 10-12 mm of eyelid elevation
■ Embryology: Develops in the third gestational month from the superior rectus muscle
■ Anterior lamella of the levator muscle forms aponeurosis
■ Posterior lamella of the levator muscle forms Müller muscle
■ Approximately 2-5 mm above the tarsus the anterior portion of the levator aponeurosis joins the orbital septum.
MÜLLER MUSCLE
■ Origin: Posterior lamella of levator muscle
■ Insertion: Superior border of tarsus
■ Innervation: Sympathetics
■ Action: Provides 2-3 mm of eyelid elevation
FRONTALIS MUSCLE
■ Origin: Galeal aponeurosis
■ Insertion: Suprabrow dermis
■ Innervation: Frontal branch of facial nerve
■ Action: Elevates brow and upper eyelid skin
ETIOLOGIC FACTORS/PATHOPHYSIOLOGY2,3
TRUE PTOSIS
■ Intrinsic drooping of the affected eyelid
PSEUDOPTOSIS: CONDITIONS THAT MIMIC TRUE PTOSIS
■ Grave disease: Retraction of contralateral lid can give appearance of ptosis on unaffected side
■ Hypotropia: Downward rotation of the globe with accompanying lid movement
■ Duane syndrome: Extraocular muscular fibrosis and globe retraction
■ Posttraumatic enophthalmos
■ Contralateral exophthalmos: Gives impression of ptosis on the unaffected side
■ Chronic squinting from irritation
CONGENITAL PTOSIS2,3
■ Developmental dysgenesis in the levator muscle
■ Idiopathic persistent ptosis noticed shortly after birth
■ Usually not progressive
■ Signs confined to the affected eyelid(s)
■ Decreased palpebral aperture with reduction of the pupil reflex to upper eyelid margin measurement (marginal reflex distance test [MRDI])
■ Decreased levator excursion
• Poor or absent levator function reflected in the absence of the supratarsal crease
■ Ptotic eyelid generally higher than the normal eyelid during downgaze
■ Inheritance pattern unclear
■ Levator biopsies in congenital ptosis show absence of striated muscle fibers with fibrosis.
TIP: History alone usually can distinguish congenital from acquired ptosis, but if there is a question, lagophthalmos on downward gaze is characteristic of congenital ptosis, because levator fibrosis prevents downward lid migration.
■ Associated ocular abnormalities
• Coexistent strabismus and amblyopia
► Caused by pupil occlusion
• Marcus Gunn jaw-winking syndrome
► Synkinesis of upper lid with chewing
► Seen in 2%-6% of congenital ptosis
► Caused by aberrant innervation from fifth cranial nerve
• Blepharophimosis syndrome
► Triad of ptosis, telecanthus, and phimosis of lid fissure
• Congenital anophthalmos or microphthalmos
► Hypoplasia of the lids, globe, and orbital bones
• Coexistent eyelid hamartoma
► Neurofibromas
► Hemangiomas
► Lymphangiomas
ACQUIRED PTOSIS2,3
■ Myogenic
• Involutional myopathic (senile ptosis)
► Most common type
► Stretching of the levator aponeurosis attachments to the anterior tarsus
► Dermal attachments are maintained and therefore the supratarsal crease rises.
► Levator function is usually good.
• Chronic progressive external ophthalmoplegia
► Progressive muscular dystrophy affects the extraocular muscles and levator.
► 5% of cases involve the facial and oropharyngeal muscles.
■ Traumatic
• Second most common type
• Allow recovery of myoneural dysfunction, resolution of edema, and softening of scar (approximately 6 months).
• This can occur after cataract surgery from dehiscence of levator aponeurosis.
■ Neurogenic
• Third nerve palsy: Paralyzes levator muscle
• Horner syndrome: Paralyzes Müller muscle
• Myasthenia gravis
► Primarily, young women and old men are affected.
► Ptosis worsens with fatigue, at the end of the day.
► Improvement with neostigmine or edrophonium is characteristic.
■ Mechanical
• Upper lid tumors
• Severe dermatochalasis (excessive upper lid skin), brow ptosis
EVALUATION2,3
DETERMINATION OF CAUSE
■ Congenital or acquired
TIP: Evaluate for lagophthalmos during downward gaze. This indicates levator fibrosis, which is more commonly seen with congenital cases.
DEGREE OF PTOSIS (Table 39-1)
Table 39-1 Degree of Ptosis

■ Always compare with contralateral side.
■ Measure amount of descent over upper limbus.
• 1-2 mm: Mild
• 3 mm: Moderate
• 4 mm or more: Severe
■ Record palpebral fissure height.
LEVATOR FUNCTION (Table 39-2)
Table 39-2 Levator Function

■ Measure from extreme downward gaze to extreme upward gaze while immobilizing the brow.
■ >10 mm: Good
■ 5-10 mm: Fair
■ <5 mm: Poor
PREOPERATIVE EVALUATION FOR DRY-EYE SYMPTOMS
■ Schirmer tests I and II (see Chapter 34)
■ Bell phenomenon: Upward rotation of globe when eyes forcibly opened, corneal protective mechanism during sleep
■ Tear film breakup and tear lysozyme electrophoresis: Advanced ophthalmologic tests useful to further characterize causes of dry-eye symptoms
TIP: General rule: If contact lenses can be worn, then tear production is adequate.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


