Bipedicled Nasal Septal Mucosal Flaps
D. N. F. FAIRBANKS
G. R. FAIRBANKS
Medical folklore suggests nose picking to be a common cause of septal perforations, but septal operations appear to be the far more frequent offender at present. Intranasal cryosurgery and cautery for epistaxis, when performed bilaterally and simultaneously in corresponding areas, also can lead to perforations. Nasal septal abscess, which usually forms after untreated posttraumatic septal hematoma, syphilis, tuberculosis, Wegener’s granulomatosis, and cocaine abuse, also can cause perforations.
A combined technique of bipedicled mucosal advancement flaps fortified with a temporalis fascia autograft is a good method of closing perforations (1).
INDICATIONS
The perforated nasal septum vexes both the patient and the physician (Fig. 76.1). It commonly causes intranasal crusting and epistaxis, and it occasionally causes whistling, particularly when the perforation is small. While these may be minor annoyances for some patients, for others they are major handicaps.
The nonoperative treatment of nasal septal perforations will not be discussed in this chapter (2, 3). Surgical techniques reported in the literature for closure are varied and ingenious. However, advancement of viable tissue into a hole is indeed a difficult surgical challenge, one plagued by slough and reperforation often several months or years postoperatively. Many surgeons are still pessimistic regarding the probability of successful surgical closure.
Septal perforations can be closed with bipedicled advancement flaps of nasal mucosa designed to maximize the vascular supply of the septum (Fig. 76.2). The repair is then fortified by the submucosal insertion of a temporalis fascial or pericranial autograft. The graft increases the success of the repair, even when complete mucosal closure is difficult.
ANATOMY
A bipedicled flap of septal mucosa is designed so that the incisions along the nasal dorsum and nasal floor run parallel to the blood supply (4). The arteries that supply these flaps, through interconnecting anastomoses, are the anterior ethmoid, the posterior ethmoid, and the sphenopalatine (Fig. 76.2).
 FIGURE 76.1 Cross section of the nose through a perforation in the cartilaginous septum. (From Fairbanks, ref. 5, with permission.) |
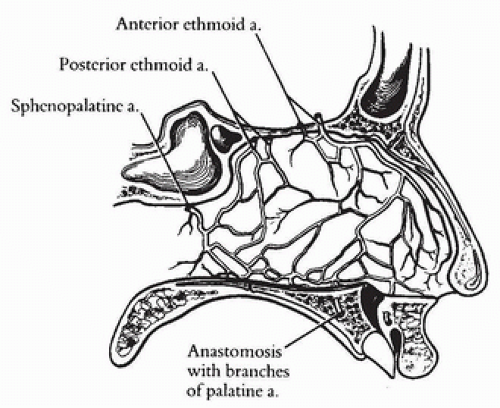 FIGURE 76.2 Arterial supply of the nasal septum. (From Gollom, ref. 4, with permission.)
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Oral Mucosal Flaps for Septal Reconstruction Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap) Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|