Nail phenolization is considered a useful procedure for treating ingrowing toenails. Nail phenolization is indicated when partial and definitive removal of the nail plate is necessary. Nail phenolization is simple and inexpensive, and associated with little postoperative discomfort, a quick return to normal activities, and a low rate of complication and recurrence. The Howard-Dubois and super U techniques are indicated when ingrowing nails are caused by hypertrophy of nail folds, according to the degree of severity.
Key points
- •
Nail phenolization is considered a useful procedure for treating ingrowing toenails.
- •
Nail phenolization is indicated when partial and definitive removal of the nail plate is necessary.
- •
Nail phenolization is simple and inexpensive, and associated with little postoperative discomfort, a quick return to normal activities, and a low rate of complication and recurrence.
- •
The Howard-Dubois and super U techniques are indicated when ingrowing nails are caused by hypertrophy of nail folds, according to the degree of severity.
- •
The Howard-Dubois and super U techniques produce very good results, although the healing time and time until return to normal activities are longer with the super U technique.
An ingrown toenail is a common problem that causes significant morbidity and disability in daily life. An imbalance between the widths of the nail plate and the nail bed and the hypertrophy of nail folds are considered to be the causes. A large number of articles on the conservative treatment of ingrowing toenails have been described. Techniques such as massaging the nail folds, taping, gutter splinting, and orthesis may help in the treatment of ingrowing nails, especially in mild cases and in children. These treatments are lengthy and, when they are not well indicated, recurrence rates are considered high. Surgical treatment is indicated either when conservative treatments have failed or in moderate and severe cases. For cases in which nail is responsible for the ingrown toenail, the definitive narrowing of the nail plate is preferred. When the condition is caused by hypertrophy of nail folds, debulking of the periungueal soft tissues is performed. This article describes the best surgical treatment of ingrowing toenails.
Narrowing of the nail plate
Nail phenolization is the best technique for definitive narrowing of the nail plate. It is well indicated in patients with diabetes and those using anticoagulants. Patients should be advised about the postoperative oozing and inflammatory process of proximal and lateral nail folds, and normal daily activities.
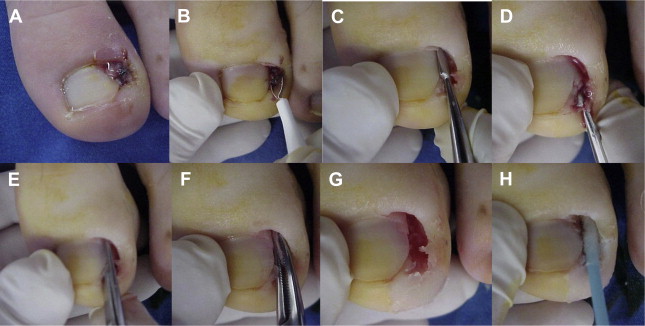
Nail phenolization is considered easy to perform, but specialized training is required. After cleaning the involved digit with alcohol 70%, a tourniquet is applied and distal block anesthesia with lidocaine 2% without epinephrine is administered. When granulation tissue is present, it should be curetted to enable a better view of the nail plate to avoid excessive nail plate removal. The lateral involved nail plate is detached from the nail bed and the lateral and proximal nail folds (≈3–5 mm). The nail plate is split using a scissors or nail nippers from the free edge to the matrix and removed using a hemostat in a rotation motion. When necessary, the nail matrix, nail bed, and lateral nail fold are gently curetted to remove debris. A cotton swab is moistened with phenol solution 88% and applied to the lateral sulcus under the proximal fold and rubbed vigorously onto the matrix for 1 minute ( Fig. 1 ).
Management of Complications
Oozing appears on the third day and may continue for up to 3 weeks. This oozing is improved by frequent washing of the wound, at least twice a day. A 20% ferric chloride solution can be used just after phenolization to improve postoperative drainage. Slight edema in the lateral and proximal nail folds may remain for 1 week, and can be improved by applying clobetasol cream. Infection, although rare, is the most common complication. An antibiotic is indicated in the case of postoperative infection. Unnecessary burn of proximal and lateral nail folds appears when the cotton swab is excessively moistened; the applicator must be moistened with phenol solution, but not dripping. Postoperative periostitis may occur when the nail matrix is strongly curetted. This procedure, when necessary, must be performed gently. Excessive detachment of the nail plate plus a dripping applicator may result in a temporary or definitive nail dystrophy. Care must be given to detach just the necessary lateral part of the nail plate.
Postprocedural Care
The limb should be elevated for 1 day. The dressing should be removed after 24 hours and the wound cleaned with 3% hydrogen peroxide. The patient should be advised to wash the wound twice a day and avoid closed shoes until the oozing disappears. The wound should be covered with a simple bandage. Patients should return for follow-up the next day and in 10, 30, and 60 days.
The clinical results and a review of the literature are summarized in Table 1 .
| Author, Year | Number of Surgeries | Follow-up (mo) | Recurrence Rate (%) |
|---|---|---|---|
| Kimata et al, 1995 | 537 | 6 | 1.1 |
| Bostanci et al, 2001 | 350 | 25 | 0.6 |
| Andreassi et al, 2004 | 948 | 18 | 4.3 |
| Di Chiacchio et al, 2010 | 267 | 33 | 1.9 |
Outcomes
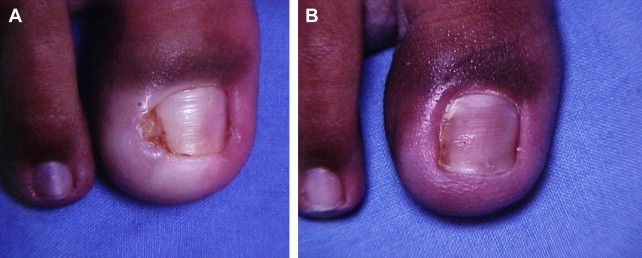
The results of nail phenolization are considered excellent, both functionally and cosmetically ( Fig. 2 ).
Narrowing of the nail plate
Nail phenolization is the best technique for definitive narrowing of the nail plate. It is well indicated in patients with diabetes and those using anticoagulants. Patients should be advised about the postoperative oozing and inflammatory process of proximal and lateral nail folds, and normal daily activities.
Nail phenolization is considered easy to perform, but specialized training is required. After cleaning the involved digit with alcohol 70%, a tourniquet is applied and distal block anesthesia with lidocaine 2% without epinephrine is administered. When granulation tissue is present, it should be curetted to enable a better view of the nail plate to avoid excessive nail plate removal. The lateral involved nail plate is detached from the nail bed and the lateral and proximal nail folds (≈3–5 mm). The nail plate is split using a scissors or nail nippers from the free edge to the matrix and removed using a hemostat in a rotation motion. When necessary, the nail matrix, nail bed, and lateral nail fold are gently curetted to remove debris. A cotton swab is moistened with phenol solution 88% and applied to the lateral sulcus under the proximal fold and rubbed vigorously onto the matrix for 1 minute ( Fig. 1 ).





