Bell’s palsy is unilateral, acute onset facial paralysis that is a common condition. One in every 65 people experiences Bell’s palsy in the course of their lifetime. The majority of patients afflicted with this idiopathic disorder recover facial function. Initial treatment involves oral corticosteroids, possible antiviral drugs, and protection of the eye from desiccation. A small subset of patients may be left with incomplete recovery, synkinesis, facial contracture, or hemifacial spasm. A combination of medical and surgical treatment options exist to treat the long-term sequelae of Bell’s palsy.
Key points
- •
Bell’s palsy describes an acute, unilateral facial paralysis believed to be caused by herpes simplex virus.
- •
It is most commonly found in people 15 to 45 years of age and occurs in 1 in 65 people in a lifetime.
- •
Medical treatment of Bell’s palsy involves oral steroid and measures to protect the eye from desiccation.
- •
Most patients with Bell’s palsy have spontaneous resolution.
- •
Patients who do not resolve completely may need further treatment to improve facial function, and manage secondary sequelae such as synkinesis, hypertonicity, or facial asymmetry.
Introduction
Accounts of facial paralysis date back to 5th century BCE by Hippocrates. Sir Charles Bell described the anatomy of the facial nerve and its association with unilateral facial paralysis in 1821. Since then, idiopathic facial paralysis has been termed Bell’s palsy. Bell’s palsy describes an acute, unilateral facial paralysis. This entity is a clinical diagnosis after exclusion of the other etiologies of facial paralysis through an astute patient history, physical examination, and laboratory or imaging studies if necessary. It is essential to understand that not all facial paralyses are Bell’s palsy because a patient’s management is driven by an identifiable etiology if one exists. Bell’s palsy is defined by rapid onset, unilateral, lower motor neuron type of facial deficit, with lack of central nervous system, otologic, or cerebellopontine angle diseases. However, patients may have additional symptoms of hyperacusis, change in taste, facial sensation or pain, and epiphora. The facial paralysis can be partial or complete, although it is often self-limited. It can occur in women, children, and men; however, it is more common in people 15 to 45 years of age. Patients with compromised immune systems, diabetes, and those who are pregnant are at higher risk. The resulting facial paralysis can have devastating implications for a patient’s function and appearance. Identification and management of patients to optimize return of facial function is crucial.
Introduction
Accounts of facial paralysis date back to 5th century BCE by Hippocrates. Sir Charles Bell described the anatomy of the facial nerve and its association with unilateral facial paralysis in 1821. Since then, idiopathic facial paralysis has been termed Bell’s palsy. Bell’s palsy describes an acute, unilateral facial paralysis. This entity is a clinical diagnosis after exclusion of the other etiologies of facial paralysis through an astute patient history, physical examination, and laboratory or imaging studies if necessary. It is essential to understand that not all facial paralyses are Bell’s palsy because a patient’s management is driven by an identifiable etiology if one exists. Bell’s palsy is defined by rapid onset, unilateral, lower motor neuron type of facial deficit, with lack of central nervous system, otologic, or cerebellopontine angle diseases. However, patients may have additional symptoms of hyperacusis, change in taste, facial sensation or pain, and epiphora. The facial paralysis can be partial or complete, although it is often self-limited. It can occur in women, children, and men; however, it is more common in people 15 to 45 years of age. Patients with compromised immune systems, diabetes, and those who are pregnant are at higher risk. The resulting facial paralysis can have devastating implications for a patient’s function and appearance. Identification and management of patients to optimize return of facial function is crucial.
Facial nerve anatomy
The complex anatomy of the facial nerve is relevant to understanding its function. In general, there are 3 portions of the facial nerve—the intracranial portion, the intratemporal portion, and the extratemporal portion. The facial nerve exits the brainstem at the cerebellopontine angle and enters the internal auditory canal of the temporal bone. In the internal auditory canal, it is accompanied by the VIIIth cranial nerve. Within the temporal bone there exist various segments of the nerve from the labyrinthine segment, the geniculate ganglion, tympanic segment and the vertical (mastoid) segment. Within the temporal bone, the first 3 branches are the greater superficial petrosal nerve, which provides secretomotor fibers to the lacrimal gland and conveys taste from the soft palate; the nerve to the stapedius muscle, which is involved in dampening sound vibrations, and chorda tympani nerve, which conveys taste fibers from the anterior two-thirds of the tongue and supplies secretomotor fibers to the sublingual and submandibular glands. The nerve then exits the stylomastoid foramen and branches further in the extratemporal portion of it. The nerve gives off the posterior auricular nerve branch as well as branches to the posterior belly of the digastric and stylohyoid muscles. The main trunk of the facial nerve is found within the parotid gland, where it further divides into a frontozygomatic (upper) and cervicofacial (lower) division at the pes anserinus (“goose’s foot). After that division the nerve divides into 5 major branches: the frontal, zygomatic, buccal, marginal mandibular, and cervical. These nerve branches go on to innervate the muscles of facial expression.
Incidence
Bell’s palsy is found fairly equally in males and females, but there tends to be a slightly greater occurrence in men older than 40 years old and in women younger than 20. In general, the greatest incidence is seen in the 15- to 45-year-old age group. In the general population, the incidence ranges from 11.5 to 40.2 per 100,000. In the United States, the incidence ranges from 25 to 30 per 100,000, in Japan, it is reported as 30 per 100,000, and in the United Kingdom, and it is 20.2 per 100,000. This disease affects approximately 1 in 65 people in a lifetime. On presentation, 70% of patients with Bell’s palsy have complete paralysis and 30% have incomplete paralysis. Bell’s palsy affects the right and left sides of the face fairly equally. Bilateral paralysis is rare and occurs in 0.3% of patients. A personal history of Bell’s palsy is found in 9%, and a family history of Bell’s palsy is found in 8% of patients. There is a greater incidence of Bell’s palsy in patients with diabetes, hypertension, immunocompromised status, after upper respiratory viral infection, and in pregnancy. Most patients with Bell’s palsy experience spontaneous resolution; 84% have near normal facial function and 71% resolve completely. In patients with incomplete paralysis, 94% recover completely within 4 months of onset. However, only 61% of patients with complete paralysis have complete recovery. Those who do not recover may be left with persistent facial weakness, synkinesis, or facial contracture. Synkinesis is defined as unintentional movement of a segment of the face during volitional movement of another segment.
Etiology
Numerous etiologies have been proposed for Bell’s palsy, such as autoimmune disorders, infections, ischemic insults, and hereditary. The most generally accepted etiology, however, is that of the herpes simplex virus (HSV-1) inducing edema of the facial nerve that results in the facial dysfunction seen in patients with Bell’s palsy. HSV-1 enters the body through mucocutaneous contact and has an affinity for peripheral nerves. The virus can lay dormant in the ganglia of peripheral nerves until it is reactivated. The DNA of HSV-1 along with varicella zoster has been identified in endoneural fluid in patients with Bell’s palsy. Histopathologic studies of temporal bones of patients with Bell’s palsy have also shown infiltration of lymphocytes and associated demyelination or axonal degeneration surrounding the facial nerve. Although the viral etiology of Bell’s palsy is accepted, given the circumstantial evidence, the exact etiology still is considered to be unclear. Risk factors for the development of Bell’s palsy have been identified, and include pregnancy, severe preeclampsia, diabetes, upper respiratory tract infections, and hypertension, as well as obesity.
Diagnosis
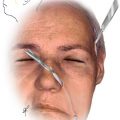
Bell’s palsy is a clinical diagnosis and is largely one of exclusion. Patients present with a sudden onset of facial weakness that tends to be unilateral and rapidly progressive. The facial weakness tends to reach its peak within 72 hours. Patients may also have accompanied hyperacusis, change in facial sensation, neck or periauricular pain, or dysgeusia. In some patients, pain tends to precede palsy; patients may feel a sense of fullness of the ear or ear pain before manifesting facial weakness. However, if pain is significant and accompanies Bell’s palsy, the patient is believed to have the diagnosis of Ramsey–Hunt syndrome, which is thought to be caused by varicella zoster infection. Additionally, with the loss of facial function, patients have incomplete eye closure, which can result in corneal exposure and desiccation. A Bell’s phenomenon has been described as an upward rotation of the globe when patients attempt to close their eyes. This, however, is only present in 75% of the population ( Fig. 1 ). Moreover, in Bell’s palsy, the associated loss of the orbicularis oculi muscle function impairs the adequate handling of tears. Patients tend to have epiphora owing to an ineffective pump mechanism to spread the tear film, combined with irritation of the eye itself. With the loss of facial muscular tone, the eyebrow along with the middle and lower face droop, giving patients the appearance that they have had a stroke. This can have a significant, negative impact on a person’s self-image and the way they interact with others in society. Loss of function of the frontalis muscle results in immobility of the eyebrow and eventual brow ptosis that gives the impression of unhappiness and can limit one’s visual field. Patients lose the ability to control their lips and mouth, thereby affecting their speech as well as their ability to eat and drink appropriately. Patients also may have trouble pronouncing certain words that have the letter b or p in them. Furthermore, they lose their ability to appropriately handle a food bolus, as well as saliva, thereby resulting in drooling or biting their own buccal mucosa. In addition to these functional deficits, patients with facial paralysis lose their ability to express themselves, such as with smiling. Consequently, the facial paralysis can have a significant negative impact on one’s psychosocial well-being.

The differential diagnosis of facial paralysis is extensive and can be divided into broad categories of congenital, cerebrovascular, infectious, neoplastic, inflammatory or autoimmune, and traumatic. The clinician’s history and physical examination is directed toward eliminating diseases within this differential diagnosis to diagnose a patient with Bell’s palsy ( Box 1 ).
Idiopathic
- •
Bell’s palsy
Infectious
- •
HIV infection
- •
Lyme disease
- •
Poliomyelitis
- •
Meningitis/encephalitis
- •
Herpes
- •
Varicella zoster (Ramsay Hunt)
- •
Epstein–Barr virus
- •
Mumps
- •
Rubella
- •
Otitis media
Trauma
- •
Soft tissue trauma
- •
Temporal bone fracture
- •
Surgery
- •
Birth trauma
- •
Barotrauma
Autoimmune disease
- •
Guillain–Barre
- •
Melkersson–Rosenthal
- •
Multiple sclerosis
- •
Amyloidosis
- •
Sarcoidosis
Neoplasm – malignant, benign, primary, metastatic
- •
Acoustic neuroma
- •
Facial nerve tumor
- •
Neurofibroma
- •
Hemangioma
- •
Glomus tumor
- •
Parotid tumor
- •
Central nervous system tumor, that is, meningioma
- •
Head and neck cancer
- •
Squamous cell carcinoma
- •
Rhabdomyosarcoma
- •
Metastatic cancer (breast, lungs, kidney, colon, skin)
Congenital
- •
Mobius syndrome
- •
Congenital unilateral lower lip paresis
- •
Hemifacial macrosomia
- •
CHARGE (coloboma, heart defects, atresia of the choanae, retardation of growth and development, genital and urinary abnormalities, ear abnormalities and/or hearing loss)
- •
VACTERL (vertebral, anal atresia, cardiac, trachea, esophageal, renal, and limb defects)
- •
Chapple syndrome
- •
Branchiootorenal
- •
Nonsyndromic
- •
Mononeural agenesis
- •
Congenital absence of facial musculature
- •
Poland syndrome
- •
Thalidomide
Otologic
- •
Acute otitis media/mastoiditis
- •
Chronic otitis media
- •
Cholesteatoma
Intracranial
- •
Stroke
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


