5. Basics of Anesthesia for the Aesthetic Surgery Patient
Deborah Stahl Lowery, Jeffrey E. Janis
GENERAL PRINCIPLES1,2
■ Anesthesia for patients undergoing purely elective aesthetic procedures presents specific challenges that encompass:
• Patient selection
• Surgical venue selection (ambulatory surgery centers, offices, hospital)
• Choice of anesthetic technique(s)
• Personnel requirements
• Postoperative care and pain management
• Discharge criteria
• Patient satisfaction
■ Requires high level of understanding, communication, and cooperation between surgeon and anesthesia provider to ensure optimal surgical outcome and patient experience
■ Regulatory agencies establish minimum standards of care in aesthetic surgery environments.
• Accreditation Association for Ambulatory Health Care (AAAHC)
• The Joint Commission (TJC), formerly Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
• American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF)
• Regulations may vary with regard to state and type of facility.
■ Professional societies provide consensus statements, guidelines, recommendations, practice parameters, and advisories for evidence-based best practices for ambulatory surgery centers (ASC) and office-based practices.
• American Society of Anesthesiologists (ASA)
• Society for Ambulatory Anesthesia (SAMBA)
• American Society of Regional Anesthesia and Pain Medicine (ASRA)
• American College of Cardiology and American Heart Association (ACC/AHA)
• American College of Surgeons (ACS)
• American Society of Plastic Surgeons (ASPS)
• American Society for Aesthetic Plastic Surgery (ASAPS)
ANESTHETIC GOALS3
■ Anxiolysis
■ Amnesia
■ Analgesia
■ Sedation
■ Unconsciousness or hypnosis
■ Immobility, including muscle relaxation or paralysis
■ Quiet, nondistracting operating milieu, if patient awake
■ Attenuation of autonomic responses to noxious stimuli
■ Preservation of vital functions
OBJECTIVES OF ANESTHESIA IN THE AESTHETIC PATIENT2
■ Safe implementation of chosen technique
■ Fast-track characteristics with rapid onset and emergence
■ Predictable and reliable methodology
■ Prevention of undesirable side effects
■ Confidence in ability to meet accepted discharge criteria
■ Patient satisfaction commensurate with entirely elective, often self-funded, procedures
TECHNIQUES2–8
General Anesthesia
■ “Balanced” technique incorporates multiple classes of IV drugs (sedative-hypnotics, narcotics, muscle relaxants), along with the volatile/inhalational agents (desflurane, sevoflurane, less commonly isoflurane and nitrous oxide).
■ Volatile agents
• Easier titration of depth, faster emergence, and early recovery
• Lesser risk of intraoperative awareness
• Simple administration
• Typically less expensive maintenance agent
Total Intravenous Anesthesia (TIVA)
■ Component therapy involving sedative-hypnotic infusion (propofol, ketamine, dexmedetomidine)
• Additional drugs such as midazolam, choice of narcotic, or muscle relaxant supplemented either by IV bolus or infusion
• Aided by liberal surgical use of local anesthetic block or infiltration
■ Reduced incidence of postoperative nausea and vomiting (PONV)
■ High degree of patient satisfaction
■ More complex administration
■ Increased cost
■ Avoids gas delivery systems and therefore need for scavenging equipment
■ Avoids malignant hyperthermia (MH) triggers (see Malignant Hyperthermia section later in the chapter)
■ Various well-described “recipes” for TIVA5,6,8 commonly include:
• Propofol: Sedation/hypnosis
• Midazolam: Anxiolysis and amnesia
• Ketamine: Dissociation and analgesia
• Opioids (fentanyl, alfentanil, remifentanil): Analgesia
• Rocuronium: Muscle relaxation
• Dexmedetomidine: Anxiolysis, sedation, analgesia, decreased adrenergic output
• Acetaminophen: Nonopioid analgesic
• Ketorolac: NSAID
■ Frequently accompanied by use of “depth of anesthesia” or “level of consciousness” monitoring
■ Employs algorithm-driven surface EEG to calculate an “index” number that correlates with hypnotic level
■ Bispectral Index (BIS; Medtronic) commonly used in the United States
• Airway can be natural or controlled (endotracheal tube or supraglottic airway), with either mechanical or spontaneous ventilation.
Regional Anesthesia
■ Neuraxial (spinal or epidural)
■ Nerve blocks: Plexus, peripheral, paravertebral, intercostal, specific nerve branch, transversus abdominal plane (TAP), truncal, or other
■ IV sedation, at multiple and varying levels
■ Local infiltration
■ Selection determined by
• Type, extent, and duration of surgery
• Patient or surgeon preference
• Anesthesiologist experience
• Patient’s underlying medical status and/or any pertinent psychological aspects
■ Can be isolated anesthetic technique or involve combinations listed previously
IMPORTANT CONSIDERATIONS WITH ADMINISTRATION OF ANESTHETICS9
■ Standard of care for nonhospital locations should be equivalent to those of hospitals.
■ ASA Standards for Basic Anesthetic Monitoring10 (last amended 2011) must be met.
■ Emergency protocols must be established, documented, and rehearsed.
■ Transfer agreement with nearby/associated hospital for unplanned admission must be established.
■ Preoperative risk assessment and evaluation are required, including laboratory tests and specialty consultation as needed.11
■ Selection of anesthesia type with appropriate monitoring
■ Selection of appropriate model of provider(s)
• Anesthesiologist, alone or as part of anesthesia care team, with certified registered nurse anesthetist (CRNA) or, in some states, an anesthesia assistant (AA)
• CRNA supervised by surgeon
• Surgeon supervising RN whose sole responsibility is administration of ordered medication(s) and monitoring patient
■ Appropriate education, training, and certification of staff involved in all phases of patient care
■ Duration and complexity of procedure(s), especially if multiple procedures will be performed simultaneously or concurrently
■ Preoperative medications and postoperative pain control plans
■ Discharge criteria and postoperative follow-up
PREOPERATIVE SCREENING, EVALUATION, AND PATIENT SELECTION12,13
GOALS
■ Identify and optimize comorbid conditions.
■ Assess suitability for ASC or office.
■ Align anesthetic needs and resources with proposed procedure and patient needs.
■ Minimize perioperative risk.
■ Reduce delays and cancellation.
■ Assess ability for safe and timely discharge.
■ Provide education and reassurance to patients to build confidence.
TOOLS
■ Checklist-format patient questionnaire
■ Primary care physician/practitioner evaluation
■ Subspecialty consultations as needed
■ Old anesthesia records
■ In-person or phone interview with anesthesiologist or nurse
■ Video chat, Skype, or telemedicine
TIMING14
■ Process guided by
• Patient demographics
• Patients’ clinical conditions
• Invasiveness of procedure
• Nature of the health care system
■ Can be done day of surgery (DOS) if low severity of disease and procedure of low-medium surgical invasiveness, otherwise in advance
THINGS ANESTHESIOLOGISTS LIKE TO KNOW OR REVIEW
■ Up-to-date history and physical examination
■ Pertinent active medical conditions
■ Current medications and therapies in place
■ Status of optimization of current problems
■ Pertinent subspecialty consultation
■ Pertinent diagnostic studies of record
■ Pertinent psychosocial conditions
■ Surgical findings and operative plan
■ History of difficult intubation
■ History of PONV or postdischarge nausea and vomiting (PDNV) (discussed later in the chapter)
■ History of other anesthetic complications like delayed emergence, unanticipated admission, or prolonged postanesthesia care unit (PACU) stay
■ Personal or familial history suggestive of malignant hyperthermia
■ Intangibles, nuances, or needs that may affect patient’s satisfaction or experience in this highly specialized, consumer-driven patient population
IDENTIFYING RISK FACTORS
■ Red flags of unsuitability for general anesthesia in an ASC or office 2,5,9,12
• Unstable angina
• Myocardial injury within 3–6 months
• Severe cardiomyopathy
• Uncompensated heart failure
• Aortic stenosis (moderate to severe) or symptomatic mitral stenosis
• Uncontrolled or poorly controlled hypertension
• High-grade arrhythmias
• Implantable cardiac devices (pacer-dependent or defibrillator)
• Recent stroke within 3 months
• End-stage renal disease (ESRD)/dialysis
• Severe liver disease
• Awaiting major organ transplant
• Sickle cell anemia
• Symptomatic or active multiple sclerosis
• Myasthenia gravis
• Severe chronic obstructive pulmonary disease (COPD)
• Abnormal/difficult airway
• Severe obstructive sleep apnea (OSA)
• Morbid obesity
• Psychiatric status unstable, dementia
• Acute substance intoxication
• Poor functional status <4 metabolic equivalents (METs) (discussed later in the chapter)
• Mathis et al 15 (2013) suggested seven independent risk factors associated with increased 72-hour morbidity and mortality in ambulatory surgery:
1. Overweight BMI
2. Obese BMI
3. COPD
4. History of transient ischemic attack/stroke
5. Hypertension
6. Previous cardiac surgical intervention
7. Prolonged operative time
PREOPERATIVE TESTING5,9,14,16
■ The culture shift is to NO routine testing.
■ Tests should be for indication only, as per current medical conditions or per procedure.
■ Avoid baseline laboratory studies when:
• Patient is healthy
• Patient has less than significant systemic disease (ASA I or II)
• Blood loss expected to be minimal
• Procedure is designated low risk
■ Testing guidelines available from ASA, SAMBA, ACC/AHA
PREGNANCY (HCG) TEST
■ Positive pregnancy tests have been reported in 0.3%–1.3% of premenopausal menstruating females, which led to postponement, cancellation, or changes in management of 100% of the cases.14
■ Routine testing of all females within childbearing years remains controversial.
■ Evidence-based medicine is inadequate or unsupportive with regards to anesthetic exposure and teratogenic effects or other harmful effects, e.g., spontaneous abortion, stimulation of contractions, or premature birth.
■ ASA provides no consensus on routine testing versus based on clinical menstrual history.
• Recommends “offering” rather than “requiring” hCG testing
• Affords “individual physicians and hospitals the opportunity to set their own practices and policies” according to ASA Choosing Wisely initiative16
■ Many institutions perform routine point of care (POC) urine hCG on day of surgery.
■ Some institutions perform rapid qualitative serum hCG testing should urine results be equivocal or contested by patient.
HEMOGLOBIN/HEMATOCRIT (HGB /HCT) AND COMPLETE BLOOD CELL COUNT (CBC)
■ Significant blood loss anticipated (>500 ml)
■ Patients with liver disease
■ Extremes of age
■ Preexisting anemia
■ Hematologic disorders
■ Factor deficiencies
CHEMISTRIES
■ High-grade dysrhythmia, pacemaker, cardiac implantable electronic device (CIED), e.g., defibrillator
■ H/O heart failure
■ Diabetes
■ Chronic renal insufficiency (CRI) or ESRD
■ Hepatic disease
■ Poorly controlled hypertension
■ Malabsorption/malnutrition (note history of eating disorder or bariatric surgery)
BLOOD GLUCOSE
■ In diabetics, obtain by blood draw as preadmission testing (PAT) or by point of care testing on day of surgery
■ HbA1C is helpful in perioperative glucose interpretation and management
COAGULATION STUDIES (PT, PTT, INR)
■ Bleeding disorders
■ Liver disease
■ Factor deficiencies
■ Chemotherapy
ELECTROCARDIOGRAM (ECG)14,17 (Box 5-1)
Box 5-1 WHEN TO OBTAIN A PREOPERATIVE ELECTROCARDIOGRAM
• Patient with known CAD or risk factors
• Patient for high risk (>1%) surgery
• Patient with known arrhythmias (helpful to have a baseline)
• Patient with known peripheral or cerebral vascular disease
• Patient with significant structural heart disease
• Patient with signs or symptoms of active cardiac conditions, e.g., chest pain, diaphoresis, shortness of breath (SOB), dyspnea on exertion (DOE)
• Patient with DM requiring insulin or end-organ damage
• Patient with renal insufficiency
■ Based on cardiac risk
■ Not indicated for asymptomatic patients undergoing low-risk surgery, regardless of age (ACC/AHA 2014)
■ Moderate-risk cosmetic procedures (abdominoplasty, large-volume liposuction, or body contouring after massive weight loss) with at least one clinical risk factor supports obtaining baseline or current/updated ECG.
■ ECGs valid for 6 months, if patient clinically stable
■ Revised Cardiac Risk Index (RCRI) clinical risk factors:
• Coronary artery disease (CAD) with H/O myocardial infarction, coronary artery bypass graft (CABG) bypass, percutaneous coronary intervention (PCI), intracoronary stents
• Cerebral vascular disease, with H/O stroke or transient ischemic events
• Heart failure
• Diabetes, requiring insulin, poorly controlled, or with end-organ damage
• Renal insufficiency, serum creatinine >2.0 mg/dl or ESRD
■ RCRI stratifies risk of major cardiac complications.
• No risk factors: 0.4%
• One risk factor: 1.0%
• Two risk factors: 2.4%
• Three or more risk factors: 5.4%
Risk interpreted as:
• Patients with <1.0% are low risk and need no further testing.
• Patients with ≥1.0% are a greater risk and should be evaluated for optimization or further workup before elective surgery.
■ High-risk indicators that should command attention and dissuade from elective surgery in anything but a hospital setting, or not at all, are:
• Recent MI
• Unstable angina
• Uncompensated heart failure
• High-grade arrhythmias
• Hemodynamically significant valvular disease, e.g., aortic stenosis
■ Additional considerations used as risk factors
• Morbid obesity
• Poorly controlled hypertension
• High-grade arrhythmia, pacemaker, or implanted defibrillators
• H/O significant peripheral arterial disease
CHEST RADIOGRAPH
■ Not many indications in the elective aesthetic surgery patients
■ Active symptomatic pulmonary disease
ADVANCED CARDIOVASCULAR TESTING
■ Stress test, ECG, carotid duplex, vascular studies guided by subspecialty consultation
ASA PHYSICAL STATUS CLASSIFICATION (ASA PS)5,18–20 (Table 5-1)
Table 5-1 American Society of Anesthesiologists Physical Status Classification
| Physical Status | Description |
| Class I | Normal, healthy patient |
| Class II | Mild systemic disease |
| Class III | Severe systemic disease |
| Class IV | Severe systemic disease that is a constant threat to life |
| Class V | Moribund patient not expected to survive without operation |
| Class VI | Patient declared brain dead for organ donation purposes |
Emergency surgery (E) denotes any of the above patient classes requiring emergency operation (e.g., normal, healthy patient for surgery is class IE).
■ Used as a global descriptor of a patient’s clinical state based on history, physical examination, and laboratory data
■ Most widely used and accepted method of describing preoperative health status
■ Gross predictor of overall risk; does not assess surgical risk per se9
■ Robust predictor of postoperative morbidity and mortality
■ Validated by and incorporated in current risk assessment models18
■ Other applications include allocation of resources and anesthesia reimbursement.19
■ Limitations include subjectivity and interrater inconsistency.18
■ Recently updated by ASA 2014
• Definitions remain unchanged, but clinical examples reflect liberalization with some stable chronic severe diseases, e.g., ESRD with hemodialysis, moving from class IV to class III
■ Patients frequently present for aesthetic surgery with multiple medical problems that represent an ASA III status.
■ ASA III patients are a widely disparate group with huge variations in pathophysiology.
NOTE: The presence of stable, optimized preexisting diseases consistent with an ASA III status is NOT a contraindication for elective surgery.
NPO FASTING GUIDELINES AND PREVENTION OF PULMONARY ASPIRATION (Table 5-2)21
Table 5-2 ASA Guidelines for Fasting (in adults, updated 2011)
| Ingested Material | Minimum Fasting Period (hours) |
| Clear liquids | 2 |
| Dairy, nonclear juices | 6 |
| Light meal (toast and clear liquid) | 6 |
| Heavy meal (fried, fatty foods; meat) | ≥8 |
FASTING
■ Guidelines are limited to healthy patients undergoing elective procedures.
■ Modification based on clinical indicators may be needed.
■ Modification may be needed if difficult airway is anticipated.
■ Patients need to be informed (verbal, written) and status verified on day of surgery.
■ Following the guidelines does not guarantee sufficient gastric emptying.
NOTE: Allowing black coffee and plain tea as “clear liquid” intake per guidelines for healthy patients without aspiration concerns can have added benefit of preventing caffeine withdrawal headaches.
ACID ASPIRATION PROPHYLAXIS AND CONSIDERATIONS
■ Pulmonary aspiration: Aspiration of gastric contents occurring after the induction of general anesthesia, during a procedure, or in the immediate period after surgery
■ ASA and SAMBA recommend NO ROUTINE administration of preoperative acid aspiration prophylaxis medications.
■ Clinical indications for use of medications, AS WELL AS EXTENDING OR MODIFYING NPO GUIDELINES, incorporate comorbidities that affect or delay gastric emptying:
• Obesity
• Pregnancy
• Diabetes
• Gastroesophageal reflux disease (GERD)
• Hiatal hernia
• After bariatric surgery (especially laparotomy band)
• Ileus or bowel obstruction
• Emergency surgery (e.g., return to OR for hematoma or wound dehiscence after PO intake in PACU)
■ Preoperative prophylactic medications include:
• Gastrointestinal stimulants (metoclopramide)
• Gastric acid blockers
► H2-receptor antagonists (cimetidine, ranitidine, famotidine)
► Proton pump inhibitors (omeprazole, lansoprazole)
• Antacid, nonparticulate (sodium citrate)
• Antiemetics (ondansetron, prochlorperazine) used alone or in combination
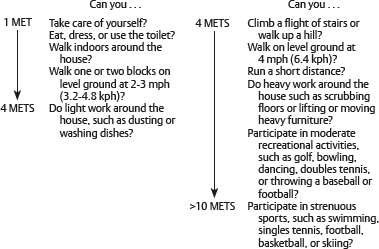
FUNCTIONAL STATUS AND METABOLIC EQUIVALENTS (METS)
FUNCTIONAL STATUS OR FUNCTIONAL CAPACITY9,17
■ Derived by estimating patient’s abilities to perform various tasks and activities of daily living (ADLs)
■ Expressed in METs
• 1 MET = 3.5 ml O2 uptake/kg/min (resting oxygen uptake in sitting position)
■ Adjunct to assess cardiac risk
■ Although not a formal component of the ASAPS classification, it is part of the routine anesthetic preoperative evaluation described as:
• <4 METs; = 4 METs; <4 METs
■ Used as an indicator on Gupta Myocardial Infarction and Cardiac Arrest (MICA) Perioperative Cardiac Risk Calculator22
■ Used as an indicator on ASC National Surgical Quality Improvement Program (NSQIP) Surgical Risk Calculator11
■ Has been suggested as a useful adjunct in assessing ASA class II-IV patients and an independent predictor of outcome and mortality23
■ Patient descriptors:
• Totally independent
• Partially dependent
• Totally dependent
POOR FUNCTIONAL STATUS
■ Has been suggested for use as an additional (downgrading) subset to the ASA PS criteria24
• <4 METs is of concern and indicates poor functional status with increased risk of cardiopulmonary complications.