Basic Principles of Facial Surgery
Suture Materials and Techniques
We use atraumatic cutting needles for the skin, and we generally use round needles for the mucosa. Our suture material of choice for the face is 6-0 or 7-0 monofilament on a very fine needle. Occasionally, we use 5-0 monofilament for areas that are not visible (Prolene, PDS, P 1 and P 6 5-0 needle with P 3 or PS 3 needle).
Our subcutaneous sutures are composed of absorbable or fast-dissolving braided or monofilament material (Vicryl or PDS, P 1, P 3 needle Ethicon, Norderstedt, Germany).
A suture or suture line must remain in place only until the wound has healed to an adequate tensile strength. Leaving sutures in for too long results in ugly scarring of the needle tracks.
Sutures are removed as early as possible. Sutures in the eyelid area or near the border of the lip should be removed on the fifth postoperative day, and sutures in other facial areas on day five or six. If sutures have been placed under tension, we remove them on day seven or eight. Sutures in the posterior auricular surface are removed on day eight.
The simple interrupted suture ( Fig. 2.1 ) is most commonly used. Each surgical knot should be tied with at least two, or preferably three, throws tied in opposite directions.
We generally use continuous sutures ( Fig. 2.2 ) for the lid area, for long traumatic wounds, and behind the ear in auricular reconstructions. After every three or four stitches, we usually tie an intermediate knot to obtain a secure coaptation.
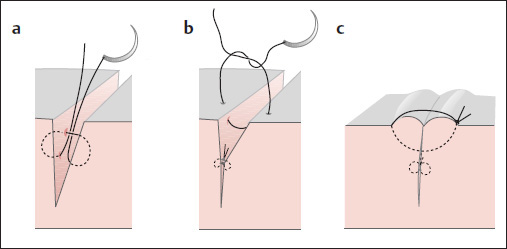
The tightened suture should raise the wound edges slightly, so that the scar will be at skin level following scar contraction. With deep wounds, a subcutaneous approximating suture is placed initially with a buried knot ( Fig. 2.1a, b ).
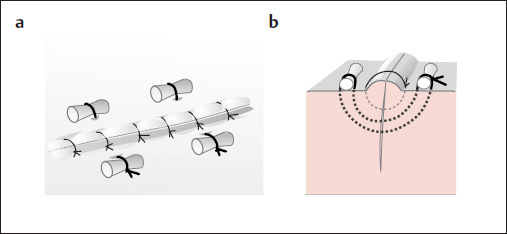
In areas where two skin incisions meet at an angle, we generally use a Donati or Allgöwer type of vertical mattress suture to coapt the wound edges ( Fig. 2.3 ).
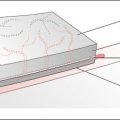
Wounds under tension are additionally reinforced with mattress sutures tied over ointment-impregnated gauze or silicone button ( Fig. 2.4 ). These sutures are removed in 7 to 10 days.
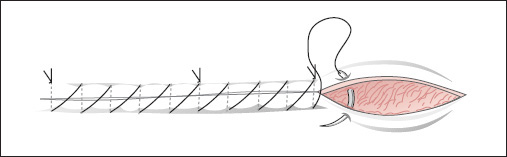
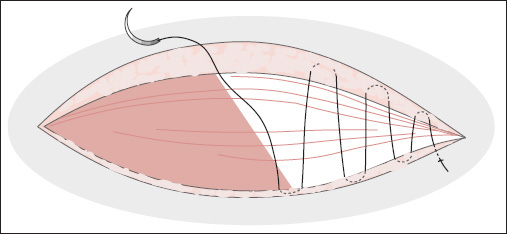
The continuous intracutaneous suture can yield a more favorable cosmetic result in many surgical procedures ( Fig. 2.5 ). We use 4-0 or 5-0 monofilament material for this type of suture.
Adhesive strips can be added to the sutures, to further relieve tension on the wound edges and ensure a cosmetically acceptable scar.
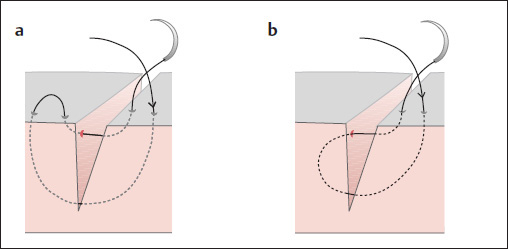
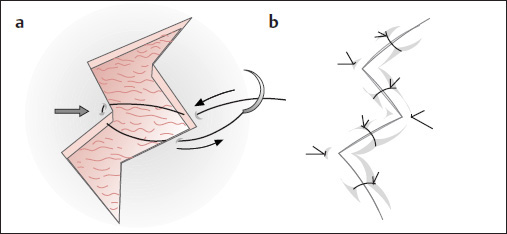
The Gillies corner suture is used in angled suture lines and for the dispersion of scars ( Fig. 2.6a ). The needle is passed subcutaneously through the wound angle and brought out on the opposite side ( Fig. 2.6b ).
Basic Instrument Set for Reconstructive Facial Plastic Surgery
(Weerda 2006; Weerda and Siegert 2012) ( Fig. 2.7 )
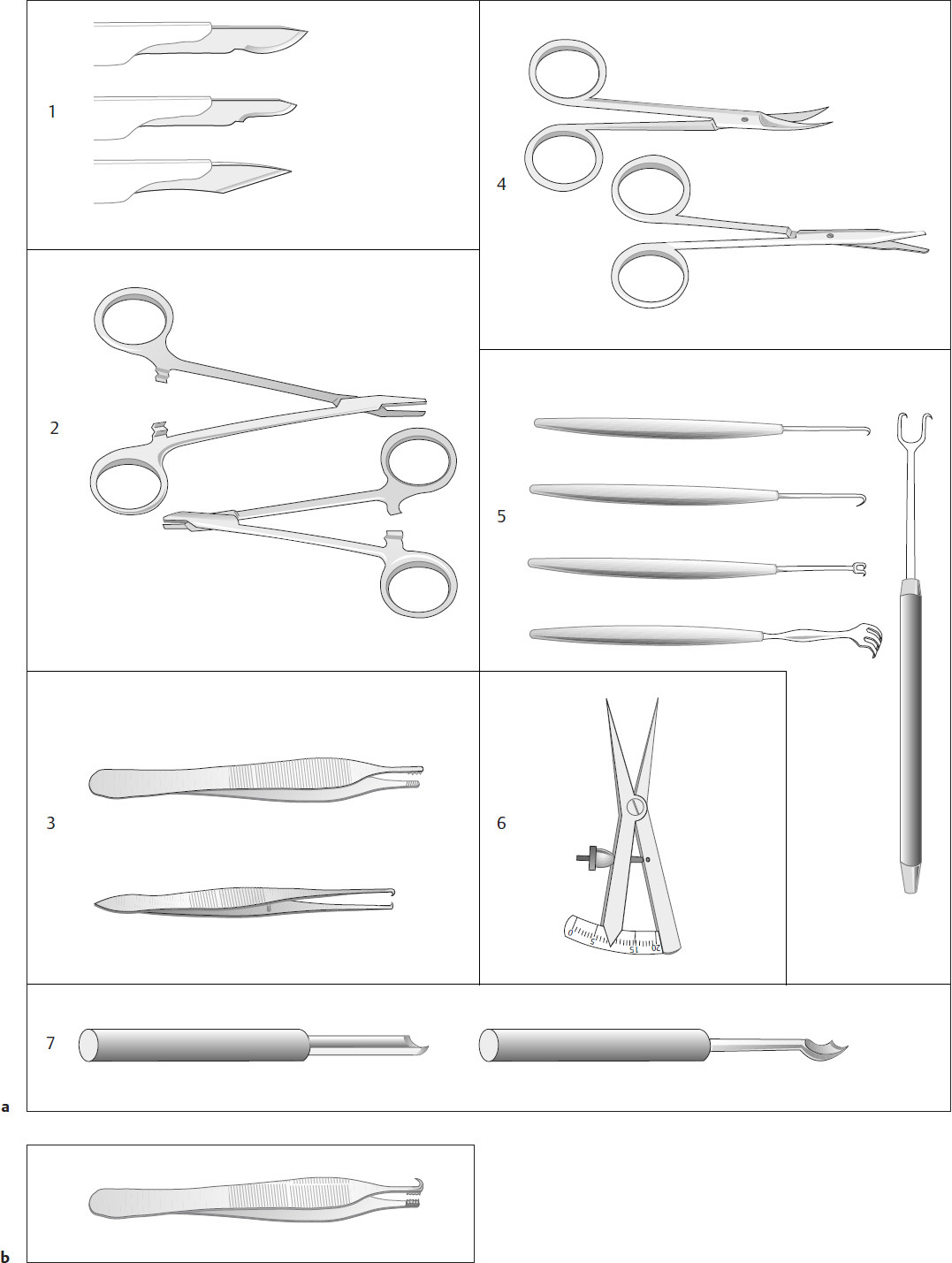
We generally use a 2× to 2.5× binocular loupe when operating and suturing. A high-quality instrument set ( Fig. 2.7a, d, e) is needed that includes no. 11, no. 15, and no. 19 knife blades ① and one small and one slightly larger needle holder for atraumatic needles ②. The set should include fine surgical forceps (e.g., Adson forceps), dissecting forceps ③, fine, angled bipolar forceps for vascular electrocautery, two or three fine hemostatic clamps, mucosal clamps, and assorted sharp-pointed scissors and dissecting scissors ④. Fine, single-prong and double-prong hooks ⑤ are useful for holding and manipulating flaps. The Weerda hook forceps ( Fig. 2.7b ) is a good alternative, but care must be taken not to crush the flap margins with the forceps. Important accessories are a millimeter rule, a caliper ( Fig. 2.7a , ⑥), and sterile color markers or methylene-blue marking pencils. Suture materials consists of 5-0, 6-0, and 7-0 monofilament, along with 4-0 and 5-0 absorbable braided and monofilament sutures. For cutting the auricular cartilage and other cartilaginous structures, we use assorted carving tools available from KARL STORZ—ENDOSKOPE, Tuttlingen, Germany ( Fig. 2.7a , ⑦ and 2.7f ; see also Figs. 11.1 and 11.3 ).
We also use various lengths of adhesive tape for dressings, and emollient ointments that often contain petroleum jelly. We routinely use suction drains and mini-suction drains to aspirate wound secretions and help contour the skin to the wound bed.
The Binocular Loupe
( Fig. 2.7c )
We have become accustomed to using a binocular loupe (2.0 to 2.5× magnification), both when performing operations and when placing sutures.
Here we will describe only the basic instrument set. The tray setups that we recommend for reconstructive facial plastic surgery are illustrated on p. 8.
The high-quality basic instrument set consists of the following items ( Fig. 2.7d ): ①) scalpels with no. 11, no. 15, and no. 19 blades; ② needle holders—one small and one slightly larger, for atraumatic needles; ③ fine tissue forceps (e.g., Adson forceps); ④ fine, angled bipolar forceps for vascular electrocautery; ⑤ two or three small hemostatic clamps; ⑥ mucosa clamps; ⑦ assorted pointed scissors; and ⑧ dissecting scissors.
We additionally use ⑨ fine, single- and double-prong hooks for holding and manipulating the flaps. A good alternative is the Weerda hook forceps ⑩ ( Fig. 2.7e ). Ordinary forceps should not be used, as they are liable to crush the flap margins. Other important accessories are a millimeter rule ⑪ and a caliper ⑫ ( Fig. 2.7f ) and sterile skin markers or methylene blue marking pencils. We use an assortment of craft knives for carving and sculpturing cartilaginous frameworks (e.g., for an auricular reconstruction; see Fig. 2.7a ⑦ and g ).
Additional instruments:
Dermatome
Mucotome
Assorted needle holders
Special clamp (or needle holder) for twisting the suture ends
Wire cutters
A Luniatschek gauze packer for burying wire sutures

Wound Management, Repair of Small Defects, and Scar Revision
Surgical procedures of up to 2.5 hours can be conducted under local anesthesia. More extensive operations and scar revisions call for general anesthesia. Care should be taken that the tape-secured endotracheal tube does not distort the face. The face should not be taped over during operations in the facial nerve area. We use a transparent film drape for this purpose (to allow facial nerve monitoring).
Relaxed Skin Tension Lines, Vascular Supply (Fig. 2.8i), and “Esthetic Units” (Fig. 2.20)
The facial surgeon must be familiar with the location and distribution of the relaxed skin tension lines (RSTLs) in the face, the facial “esthetic units” (see Fig. 2.20a–d ), and the vascular supply of the face ( Fig. 2.8i ). Besides the RSTLs, attention should also be given to wrinkle lines in the aging face.
Incisions or small excisions and sutures placed in the RSTLs will heal with fine, unobtrusive scars. Incisions and excisions made at right angles to these lines will often lead to broad, unsightly scars. Thus, the plastic surgeon should always try to place the cuts used for incisions, excisions, and scar revisions in these lines, to achieve good cosmetic results.
The term “esthetic units” (see Fig. 2.20a–d ) refers to circumscribed facial regions that should each be reconstructed as a separate unit whenever possible. The radical excision of tumors takes precedence over esthetic units, however. We shall return to this reconstructive concept in the sections that deal with specific facial regions.
Wound Management and Scar Revision
It is a general rule in facial plastic surgery to sacrifice as little skin as possible. Small wounds that extend obliquely into the tissue should be straightened whenever the surrounding tissue can be mobilized and the wound edges coapted without tension. A subcutaneous suture with a buried knot should always be placed to allow tension-free approximation of the wound margins (see Fig. 2.1 ). Because the subcutaneous tissue, epidermis, and dermis take different lengths of time to achieve adequate wound strength, early removal of the skin sutures from a wound without subcutaneous sutures would result in a broad, unsightly scar.
Management of Wounds with Traumatic Tattooing
If a wound contains embedded grit and dirt, it should first be scrubbed with a sterile toothbrush or hand brush and antiseptic soap, until all dirt residues have been removed. It can be extremely tedious to remove these particles after the wound has healed.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


