Banner-Shaped Nasal Skin Flap
J. K. MASSON
B. C. MENDELSON
EDITORIAL COMMENT
This flap should probably be considered as a first choice for many smaller nasal defects.
Most defects on the lower two-thirds of the nose are best closed with what Elliott (1) named a “banner flap,” presumably because the triangular shape of the flap resembles a banner or pennant. Although described by Elliott as a rotation flap, it is essentially the larger of two unequal flaps transposed as a type of Z-plasty (2).
INDICATIONS
The main indications for the frequent use of the banner flap are its versatility and safety, which are more recognized with increased use of the flap. Frequently, defects that are 1.5 to 2 cm in diameter have been closed, and on several occasions,
defects as large as 2.5 cm in diameter have been managed. In some circumstances, the flap has been taken from below the defect or extended onto the cheek or has been converted into a bilobed flap.
defects as large as 2.5 cm in diameter have been managed. In some circumstances, the flap has been taken from below the defect or extended onto the cheek or has been converted into a bilobed flap.
Skin grafts may have a good color match, but they leave an obvious depression. Nasolabial flaps provide an excellent color match, but the amount of subcutaneous fat and the possibility of a second stage to divide the pedicle limit their usefulness. Even then, one-fourth of the patients have required a separate defatting procedure to improve the appearance of the flap.
We believe that the larger flaps described by Rieger (3) and Lipshutz and Penrod (4) have no inherent advantage over banner flaps. In fact, they share the risks involved, in that they require more extensive mobilization of the skin. Situations requiring more complicated flaps, such as island pedicle flaps from the forehead or subcutaneous pedicle flaps from the forehead or nasolabial region, are infrequent.
ANATOMY
The terminations of the external maxillary artery form the main arterial supply and allow the successful use of many kinds of random flaps. The veins of this region empty into the anterior facial vein and also communicate through the ophthalmic vein with the cavernous sinus. The lymphatic vessels drain to the submaxillary and deep cervical lymph channels.
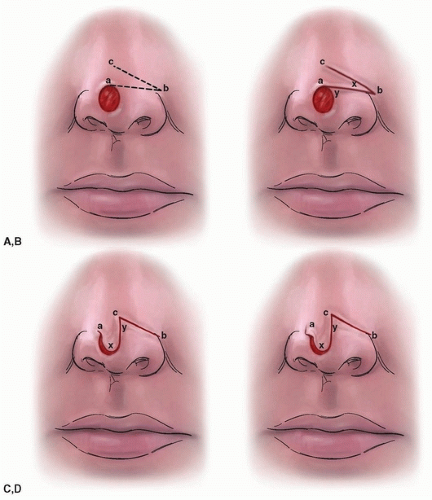 FIGURE 39.1 Principles of the banner flap procedure. A: Triangular flap is outlined by points a, b, and c. B: Larger flap x and smaller flap y. Each may be transposed as a modified Z-plasty. C: Flap y is inset, and tip of flap x is trimmed to fit the residual defect. D: The resultant dog-ear at point a, if excessive, may be reduced by a triangular excision (leaving the base untouched). (From Masson and Mendelson, ref. 2, with permission.) |
FLAP DESIGN AND DIMENSIONS
Time spent on initial outline of the best flap design is most worthwhile. The flap is outlined with a marking pen at a tangent to the edge of the defect, merging at point a (Fig. 39.1A and B). Point b is marked well out laterally and, if convenient, is placed in the alar crease, where the scar will tend to be camouflaged. However, for other than small defects, point b must be placed higher than the alar crease to minimize subsequent elevation of the nostril rim (Fig. 39.2A).
Related posts:
 Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Wraparound Cartilage Flap for Correction of Cleft-Lip Nasal Deformity
Wraparound Cartilage Flap for Correction of Cleft-Lip Nasal Deformity
 Oral Mucosal Flaps for Septal Reconstruction
Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap)
Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps
Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip
Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


