Although there are no standard guidelines for the treatment of autoimmune blistering diseases, azathioprine has shown good efficacy in acquired autoimmune blistering diseases, and is well tolerated. Side effects of azathioprine normally occur in mild variants. Severe reactions are due to reduced thiopurine S -methyltransferase (TPMT) or inosine triphosphate pyrophosphohydrolase (ITPA) activity. Therefore, screening for TPMT activity should be conducted in white patients and Africans, whereas Japanese should be screened for ITPA activity before therapy with azathioprine is started. Azathioprine is clinically meaningful for the treatment of pemphigus.
History of azathioprine
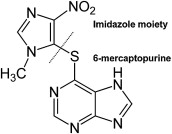
The pharmaceutical precursor of azathioprine was originally 6-mercaptopurine. 6-Mercaptopurine was synthesized in 1951 by GB Elion and GH Hitchings using techniques reported by Fisher and Traube. 6-Mercaptopurine was first used in 1953 in children with acute lymphatic leukemia. Later, Calne, a young surgeon who later became professor of surgery at Cambridge, successfully treated dogs after renal transplantation with 6-mercaptopurine in 1960, but because of the high toxic potential of the drug it was not found suitable for long-term treatment of humans with solid-organ transplants. Subsequently, it was shown that one of the derivatives of 6-mercaptopurine found by Elion and Hitchings, BW 57-322, presented with less bone marrow toxicity but was as immunosuppressive as 6-mercaptopurine. To protect 6-mercaptopurine from being rapidly metabolized, an imidazole ring had been biochemically connected via the sulfur atom at position 6 of 6-mercaptopurine and thereby azathioprine was finally developed ( Fig. 1 ). The first successful allogeneic renal transplant using a combination of azathioprine and corticosteroids was initiated in 1963. Azathioprine is now used in particular for the treatment of autoimmune diseases, such as autoimmune blistering diseases, inflammatory bowel disease, multiple sclerosis, and lupus, to name a few.
Structure and metabolism
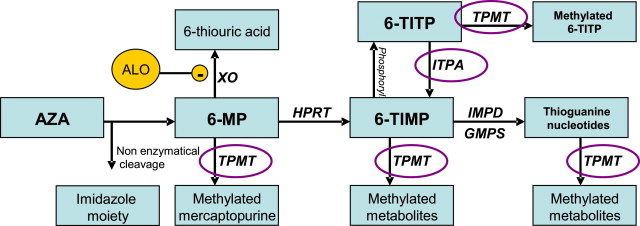
About 88% of azathioprine is ingested and 12% excreted via the gut. Nearly all the incorporated azathioprine is metabolized because only 2% is being excreted unchanged in the urine. The highest serum levels can be found approximately 2 hours after oral application and the half-life is approximately 5 hours. After uptake, azathioprine is nonenzymatically cleaved into its imidazole derivatives (methylnitroimidazole moiety) and 6-mercaptopurine (see Fig. 1 ). Three enzymes have been reported to compete for the cleavage of azathioprine ( Fig. 2 ). Thiopurine S -methyltransferase (TPMT) is able to catabolize 6-mercaptopurine into the nontoxic 6-methyl mercaptopurine. Xanthine oxidase (XO) produces the nontoxic inactive metabolite 6-thiouric acid. A lack in one of these enzymes, XO and TPMT, leads to an increased production of toxic metabolites via the hypoxanthine phosphoribosyltransferase (HPRT) pathway. A lack of TPMT activity is normally caused by genetic mutations, whereas XO might be blocked by XO inhibitory drugs such as allopurinol, which is one of the most commonly prescribed drugs in Europe and North America. The enzyme HPRT metabolizes 6-mercaptopurine into 6-thioinosine 5-monophosphate (6-TIMP). This product is processed by TPMT to active methylated metabolites or is phosphorylated to 6-thioinosine triphosphate (6-TITP). 6-TITP is converted to 6-TIMP by inosine triphosphate pyrophosphohydrolase (ITPA). A lack of ITPA, often seen in Asian populations, leads to an increase in the level of toxic 6-TITP and induces corresponding side effects, such as leukopenia, gastrointestinal disturbances, or elevated liver function test results (for details concerning side effects see later discussion).
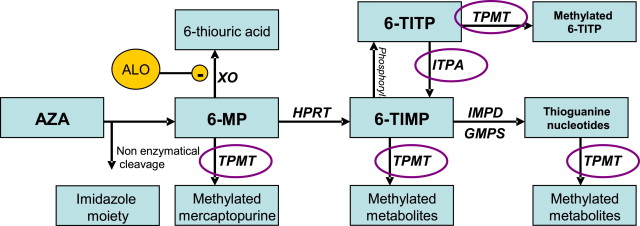
6-TIMP is converted by inosine monophosphate dehydrogenase and guanosine monophosphate synthetase into the principal active 6-thioguanine nucleotides. These nucleotides are converted by TPMT into inactive methylated metabolites.
In patients with Lesch-Nyhan syndrome, reduced expression of HPRT can be detected, which makes these patients less suitable for azathioprine treatment. Although most of the therapeutic effects of azathioprine are dependent on the HPRT pathway, there is experimental evidence that the imidazole derivatives of azathioprine might also be effective.
Structure and metabolism
About 88% of azathioprine is ingested and 12% excreted via the gut. Nearly all the incorporated azathioprine is metabolized because only 2% is being excreted unchanged in the urine. The highest serum levels can be found approximately 2 hours after oral application and the half-life is approximately 5 hours. After uptake, azathioprine is nonenzymatically cleaved into its imidazole derivatives (methylnitroimidazole moiety) and 6-mercaptopurine (see Fig. 1 ). Three enzymes have been reported to compete for the cleavage of azathioprine ( Fig. 2 ). Thiopurine S -methyltransferase (TPMT) is able to catabolize 6-mercaptopurine into the nontoxic 6-methyl mercaptopurine. Xanthine oxidase (XO) produces the nontoxic inactive metabolite 6-thiouric acid. A lack in one of these enzymes, XO and TPMT, leads to an increased production of toxic metabolites via the hypoxanthine phosphoribosyltransferase (HPRT) pathway. A lack of TPMT activity is normally caused by genetic mutations, whereas XO might be blocked by XO inhibitory drugs such as allopurinol, which is one of the most commonly prescribed drugs in Europe and North America. The enzyme HPRT metabolizes 6-mercaptopurine into 6-thioinosine 5-monophosphate (6-TIMP). This product is processed by TPMT to active methylated metabolites or is phosphorylated to 6-thioinosine triphosphate (6-TITP). 6-TITP is converted to 6-TIMP by inosine triphosphate pyrophosphohydrolase (ITPA). A lack of ITPA, often seen in Asian populations, leads to an increase in the level of toxic 6-TITP and induces corresponding side effects, such as leukopenia, gastrointestinal disturbances, or elevated liver function test results (for details concerning side effects see later discussion).
6-TIMP is converted by inosine monophosphate dehydrogenase and guanosine monophosphate synthetase into the principal active 6-thioguanine nucleotides. These nucleotides are converted by TPMT into inactive methylated metabolites.
In patients with Lesch-Nyhan syndrome, reduced expression of HPRT can be detected, which makes these patients less suitable for azathioprine treatment. Although most of the therapeutic effects of azathioprine are dependent on the HPRT pathway, there is experimental evidence that the imidazole derivatives of azathioprine might also be effective.
Azathioprine in bullous pemphigoid
In 1971, Greaves and colleagues introduced azathioprine into the treatment of bullous pemphigoid. Before that, most patients had been treated with systemic corticosteroid monotherapy to prevent recurrent blister formation. It was reported by Greaves and colleagues that in 8 of 10 patients with bullous pemphigoid, no prednisone maintenance therapy was needed for preventing relapses, whereas azathioprine was given at a dose of 2.5 mg/kg body weight per day.
In a small prospective clinical trial in 1978, Burton and colleagues examined azathioprine (2.5 mg/kg/d, n = 12) plus prednisone (30–80 mg/d) versus prednisone alone (n = 13). No significant difference between both groups was found concerning the overall disease control. The prednisone-sparing effect was statistically significant. In the azathioprine group, a cumulative average dose of 3688 mg of prednisone was used for more than 3 years, whereas 6732 mg was used in the prednisone monogroup for the same period. In 1993, Guillaume and colleagues found no significant difference in disease control between prednisone monotherapy (1 mg/kg/d, n = 31) and azathioprine (100–150 mg/d, n = 36) plus prednisone therapy. However, the prednisone-sparing effect has not been investigated in this study.
In a national randomized trial in 2007, Beissert and colleagues compared treatment with methylprednisolone (0.5 mg/kg/d) with either azathioprine (2 mg/kg/d, n = 38) or mycophenolate mofetil (1 g twice a day, n = 35). The results showed no significant differences in the primary outcome (ie, complete healing of skin lesions) and a tendency to faster healing in the azathioprine group (azathioprine 23.8 ± 18.9 days vs mycophenolate mofetil 42.0 ± 55.9 days, P value is nonsignificant). Moreover, similar corticosteroid doses were used to control disease. Mycophenolate mofetil was significantly less liver toxic compared with azathioprine, which can be an advantage especially in elderly patients.
A Cochrane review concluded from the available study results that the addition of azathioprine in the treatment of bullous pemphigoid had not been established. The results of several studies concerning the treatment of bullous pemphigoid with azathioprine are summarized in Table 1 .
| Investigators | Year | N | AZA Dose | Main Outcome |
|---|---|---|---|---|
| Greaves et al | 1971 | 10 | 2.5 mg/kg/d | 8/10 symptom free, no prednisone needed |
| van Dijk & van Velde | 1973 | 5 | 75–250 mg/d | 4/5 excellent response |
| Burton & Greaves | 1974 | 12 | 2.5 mg/kg/d | 12/12 excellent response |
| Ahmed et al | 1977 | 15 | 1.5 mg/kg/d | Reduces duration of maintenance, steroid sparing |
| Burton et al | 1978 | 12 | 2.5 mg/kg/d | Steroid sparing, but control of disease not significantly different from steroid alone |
| Guillaume et al | 1993 | 36 | 100–150 mg/d | No significant difference to steroid monotherapy concerning disease control |
| Beissert et al | 2007 | 73 | 2 mg/kg/d | No significant differences in primary outcome between AZA + MP and MMF + MP, tendency of faster healing in AZA-treated patients |
Azathioprine in pemphigus
The treatment of pemphigus vulgaris and pemphigus foliaceus usually does not differ significantly. Most investigators did not specify in their reports whether patients with pemphigus foliaceus or vulgaris had been treated.
The use of azathioprine for the treatment of pemphigus was introduced in 1969, when Krakowski and colleagues presented the first case report of a woman with pemphigus vulgaris treated successfully with azathioprine. At the same time, Aberer and colleagues published a case series of 4 patients describing the use of azathioprine as “steroid saving and beneficial” in patients with pemphigus. In 1977, Lever and Schaumburg-Lever published a retrospective analysis of 63 patients with pemphigus. The investigators treated patients (n = 12) with prednisone monotherapy and the other patients in this cohort (n = 51) with a combination of azathioprine, cyclophosphamide, or methotrexate and prednisone. In this report, azathioprine was described as “steroid saving and effective.” The investigators’ therapeutic approach is still known as Lever’s regime. Initially, patients receive a high dose of prednisone (up to 2 mg/kg body weight) in combination with azathioprine 2.0 to 2.5 mg/kg. After cessation of new blister formation and reepithelization of erosions, the prednisone dose is reduced to 40 mg/d, while the azathioprine dose remains unchanged. Further proceedings depend on the individual’s clinical development. Normally, the prednisone dose is gradually reduced over a period of several months.
There are only a few prospective randomized trials reported on pemphigus. Beissert and colleagues examined 38 patients with pemphigus vulgaris or pemphigus foliaceus and found no significant differences between treatment with azathioprine and mycophenolate mofetil, both in combination with methylprednisolone, concerning remission of disease and corticosteroid-sparing effects. The patients treated with azathioprine received a median methylprednisolone dose of 8.916 ± 29.844 mg. In the mycophenolate mofetil–treated group, patients received a median of 9.334 ± 13.280 mg methylprednisolone (n = nonsignificant). The mean duration of follow-up was 438 days in both groups. However, the time needed to achieve disease control in 50% of the patients was about 30 days in the azathioprine group compared with 75 days in the mycophenolate mofetil group. Perhaps the inhibition of at least 3 enzymatic pathways by azathioprine (see Fig. 2 ) is able to induce a faster response in comparison with mycophenolate mofetil, which inhibits primarily 1 signaling pathway. Nevertheless, after 200 days of treatment, the patients in the mycophenolate mofetil group had a remission rate of 90%, whereas those who were treated with azathioprine had a remission rate of 75%. After 600 days, this trend persisted because 20% of patients with pemphigus were still not achieving effective control with azathioprine compared with 10% of patients using mycophenolate. The recurrence rate was similar in both groups.
In another study with 120 patients analyzed, Chams-Davatchi and colleagues found no significant difference concerning disease remission between azathioprine and mycophenolate mofetil, but the patients treated with azathioprine showed significantly less steroid consumption. These findings indicate that azathioprine is well suited for first-line treatment of pemphigus. Rose and colleagues compared dexamethasone-cyclophosphamide pulse therapy with oral methylprednisolone/azathioprine therapy in pemphigus. A tendency was found in favor of methylprednisolone/azathioprine concerning complete remissions.
In IgA pemphigus, azathioprine showed no considerable effect. Dapsone is usually the first-line treatment. For pemphigus vegetans, azathioprine seems to work in individual cases. For treatment of refractory patients, disease control has been reported under the corticosteroid/azathioprine regimen using additionally photopheresis or retinoids.
In paraneoplastic pemphigus, therapy for the underlying malignancy is essential. Concomitant treatment with azathioprine and other immunomodulatory drugs has been reported, but it is difficult to conclude whether any of them will reliably affect the prognosis of the disease because its mortality approaches 90%. Lam and colleagues presented a case of a 77-year-old man with chronic conjunctivitis, acanthosis nigricans, and pemphigus-like mucocutaneous lesions. Further examinations revealed an underlying bronchogenic squamous cell carcinoma (SCC). Although skin lesions resolved with oral prednisone and azathioprine (100 mg/d) therapy, the conjunctivitis and mucous membrane erosions persisted. Verrini and colleagues described another patient with paraneoplastic pemphigus who showed good response to azathioprine (100 mg/d) but died after a short time after initiation of treatment.
The importance of systemic corticosteroids in the treatment of pemphigus is clearly documented. Because the reports show a tendency in favor of azathioprine concerning corticosteroid-sparing effects and no significant differences regarding disease control, the authors suggest using azathioprine as first-line therapy in mild to moderate cases of pemphigus. Mycophenolate mofetil seems to be a valid second-line choice. In severe and rapidly progressing cases, dexamethasone/cyclophosphamide pulse therapy should be considered.
Because pemphigus is a chronic disease, long-term follow-up studies (>3 years) are clearly needed. A Cochrane review concluded from the available study results that the optimal immunomodulatory agent in the treatment of pemphigus has not yet been found. Although azathioprine and cyclophosphamide did show advantages concerning the steroid-sparing effect, mycophenolate showed superior disease control.
The results of several studies concerning the treatment of pemphigus with azathioprine are shown in Table 2 .
| Investigators | Year | N | AZA Dose | Main Outcome |
|---|---|---|---|---|
| Krakowski et al | 1969 | 1 | 75–150 mg | Control of disease after 4 mo |
| Aberer et al | 1969 | 4 | 1–3 mg/kg/d | Steroid saving and beneficial |
| Burton et al | 1970 | 4 | 2.5 mg/kg/d | 3 of 4 with excellent response, but relapse after discontinuation of AZA; 1 patient dropped out because of severe side effects |
| Roenigk & Deodhar | 1973 | 10 | 50–250 mg/d | 7, excellent; 2, good; 1, fair |
| van Dijk & van Velde | 1973 | 5 | 50–200 mg/d | 5/5 excellent response |
| Lever & Schaumburg-Lever | 1977 | 6 | 50–150 mg/d | Steroid saving and effective |
| Lever & Schaumburg-Lever | 1984 | 21 | 100 mg/d | Safe and effective, disease control in 21 |
| Aberer et al | 1987 | 27 | 1–3 mg/kg/d | 45% free of disease; 38% clinically free of disease, but with raised antibody titers; 17% with controlled disease |
| Tan-Lim & Bystryn | 1990 | 12 | 50–150 mg/d | AZA in combination with plasmapheresis decreased antibodies faster than without plasmapheresis |
| Mourellou et al | 1995 | 15 | 100 mg/d | Remission in 14 patients, less mortality compared with steroid monotreatment |
| Carson et al | 1996 | 72 | 50–250 mg/d | AZA significantly reduced mortality, steroid sparing, 37% remission, 33% stable disease |
| Scully et al | 1999 | 17 | 1–3 mg/kg/d | Not pointed out clearly. 2 deaths reported under treatment with AZA |
| Ljubojevic et al | 2002 | 129 | 100–150 mg/d | Reduction of mortality compared with patients with steroid monotherapy |
| Beissert et al | 2006 | 18 | 2 mg/kg/d | Steroid-sparing effect of AZA similar to that of MMF. Quicker response to therapy with AZA than with MMF. No significant differences in overall outcome |
| Rose et al | 2005 | 11 | 2–2.5 mg/kg/d | Tendency in favor of AZA concerning complete remissions compared with cyclophosphamide pulse therapy |
| Chams-Davatchi et al | 2007 | 30 | 2.5 mg/kg/d | AZA most effective compared with CYP and MMF or cortisone monotherapy, but no significant differences in complete remission |
| Chaidemenos et al | 2011 | 19 | 100 mg/d | Notable steroid-sparing effect of AZA; high dose of prednisone leads significantly faster to remission than low dose of prednisone combined with AZA |
Related posts:
 Autoimmune Blistering Diseases Part II—Diagnosis and Management
Autoimmune Blistering Diseases Part II—Diagnosis and Management
 Minimizing Complications in Autoimmune Blistering Diseases
Minimizing Complications in Autoimmune Blistering Diseases
 Pemphigoid Gestationis: Current Management
Management of Linear IgA Disease
Management of Autoimmune Bullous Diseases in France: A Nationwide Network of 30 Centers
Treatment of Chronic Bullous Disease of Childhood
Pemphigoid Gestationis: Current Management
Management of Linear IgA Disease
Management of Autoimmune Bullous Diseases in France: A Nationwide Network of 30 Centers
Treatment of Chronic Bullous Disease of Childhood
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


