Axial Frontonasal Flap
D. MARCHAC
B. TOTH
This flap is a modification of the flap described by Rieger (Chapter 49) (1) with one fundamental difference. The flap described, rather than being a random-pattern flap, is an axial flap with a well-defined vascular pedicle. This allows for a much narrower pedicle and consequently more radical sliding and rotation of the nasal skin located above the defect.
INDICATIONS
The axial frontonasal flap can be adjusted more precisely with what we feel is a better cosmetic result. The donor site can be closed in a V-Y manner with the donor scar lying in a glabellar frown line. The flap is not only ideal for reconstruction of defects at the base of the nose, but more important, it is able to provide a sizable amount of skin of similar texture and color for the nasal tip as well. The scars are well hidden at the sides of the nose or in the glabellar area. The flap is not recommended when the alar margin is involved (2, 3, 4).
ANATOMY
This flap is based on a vascular pedicle located at the level of the inner palpebral ligament (Figs. 50.1 and 50.2). This pedicle is a branch of the angular artery, joining with the supraorbital arteries. It is well visualized on arteriographic studies and cadaver dissections.
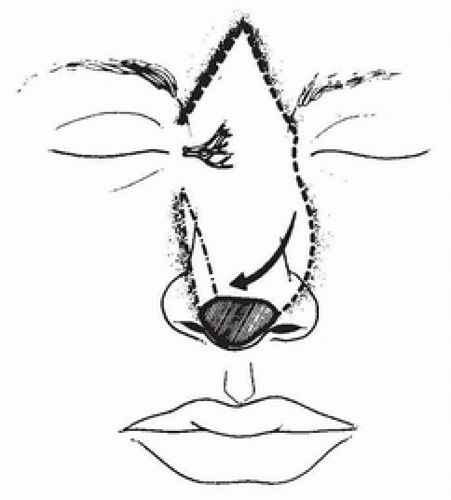 FIGURE 50.1 The axial flap is based on vessels emerging at the level of the inner canthus. This allows increased mobility and precise adjustment. (From Marchac, Toth, ref. 6, with permission.) |
FLAP DESIGN AND DIMENSIONS
Because of its axial nature, the flap can be transferred either with a narrow skin bridge or even as an island if located on the side opposite to the defect (Fig. 50.3). A curved line is drawn from the defect along the side of the nose passing medial to the canthal ligament and curving upward to follow a glabellar frown line. One should go rather high on the glabella to avoid a dog-ear when closing and then go down in a frown line on the opposite side toward the pedicle. When the defect is not centrally located, it is generally best to use the pedicle on the side of the pedicle defect since this gives the greatest flap length for reconstruction.
Related posts:
 Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Oral Mucosal Flaps for Septal Reconstruction
Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap)
Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps
Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip
Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


