54. Augmentation-Mastopexy
Purushottam A. Nagarkar
GENERAL PRINCIPLES
■ Augmentation-mastopexy is a technique used to simultaneously correct low volume and skin excess.
■ Augmentation alone corrects relative deficiency of volume.
■ Mastopexy alone corrects relative excess of skin.
■ If volume deficiency and skin excess are significant enough that either procedure alone will result in a persistent relative mismatch, combined procedure is needed.
■ The revision rate is high (8%-20%).1–3
■ Gonzales-Ulloa4 described the technique in 1960, followed by Regnault5 in 1966.
■ Surgical planning depends on relative locations of nipple and inframammary fold (IMF) (i.e., ptosis). Regnault described three categories6,7 (Fig. 54-1):
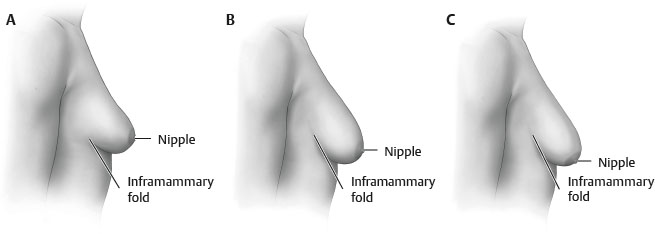
Fig. 54-1 Regnault classification of breast ptosis. A, Grade I. B, Grade II. C, Grade III.
• Grade I: Nipple at IMF
• Grade II: Nipple below IMF
• Grade III: Nipple at the lowest point on breast
■ Pseudoptosis: Nipple at or above IMF but breast parenchyma below IMF8 (Fig. 54-2, A)
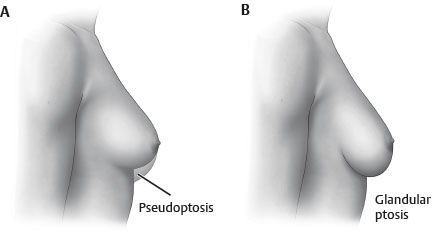
Fig. 54-2 A, Pseudoptosis. B, Glandular ptosis.
■ Glandular ptosis: Excess gland in the lower pole of the breast8 (Fig. 54-2, B)
ALTERNATIVES
AUGMENTATION ALONE
■ Use if skin excess is minimal: i.e., minimal gland below IMF, minimal ptosis, AND
■ Augmentation alone can provide appropriate projection and adequately correct ptosis by decreasing relative skin excess.
MASTOPEXY ALONE
■ Use if volume deficiency is minimal, AND
■ Skin resection alone will appropriately raise the nipple position and adequately correct projection by decreasing relative volume deficiency.
INDICATIONS
■ Ptosis (skin excess) combined with significant volume deficiency
■ Periareolar mastopexy with augmentation requires9:
• Nipple no more than 2 cm below the fold
• Nipple-areola complex (NAC) at or above breast border, not pointing inferiorly
• No more than 3-4 cm of associated breast ptosis
■ More significant ptosis will require a vertical or Wise-pattern mastopexy.
SINGLE-STAGE VERSUS TWO-STAGE PROCEDURE10
SINGLE-STAGE PROCEDURE
■ Thought to be unpredictable, with higher revision rate than that of both procedures combined11
■ One of the most common causes for malpractice claims12
• Constricted breast or skin deficiency
• Unclear whether both procedures will be necessary
► For example, no mastopexy required if patient has13:
♦ No ptosis and no pseudoptosis (<2 cm of breast parenchyma below the IMF)
♦ Alternatively, per Lee, Unger, and Adams,15 skin stretch <4 cm and nipple-to-IMF (N-IMF) distance <10 cm
• Significant asymmetry that is going to require an asymmetrical mastopexy for correction
• Significant vertical skin excess that will require a large skin resection
TWO-STAGE PROCEDURE
■ Per Lee, Unger, and Adams,15 vertical excess >6 cm is indication for staging procedure.
• If primary goal is ptosis correction, perform mastopexy first, and stage augmentation.
• If primary goal is improved projection or upper pole fullness, place implant first, and stage the mastopexy.
OUTCOMES (see Tables 54-1 and 54-2)
Table 54-1 Complication Rates for One-Stage Augmentation-Mastopexy
| Complication | Rate for Stevens et al1 (321 patients) (%) | Rate for Calobrace et al3 (235 primary augmentation-mastopexy patients) (%) | |
| Reoperation Tissue related Implant related | 14.6
3.7 10.9 Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| ||

