Chapter 2
Assessment and Management Strategy
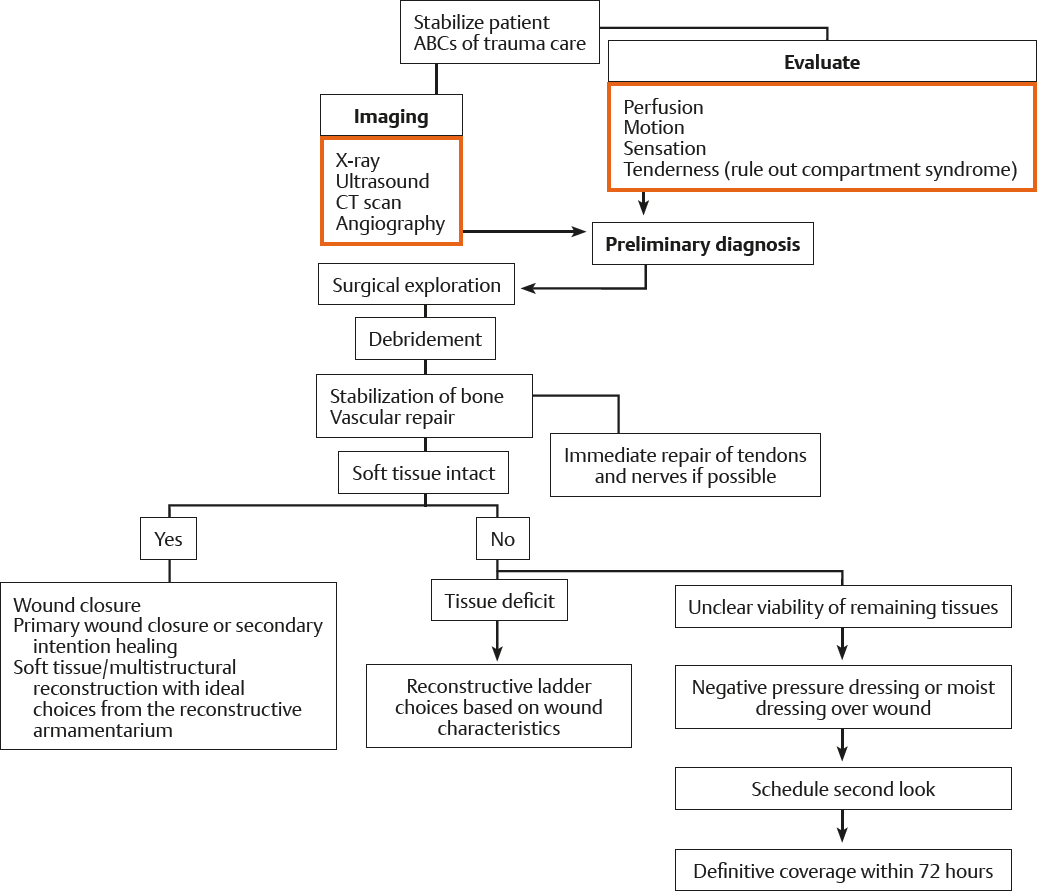
Traumatic wounds should be evaluated as soon as possible after the patient has been admitted to the emergency department. When the patient’s condition permits, an operative exploration should be performed. After adequate debridement, primary structure repair should occur if at all possible.
Patient Admission
During the first surgical exploration, all nonviable tissue is debrided. The skeleton must be stabilized first, and blood flow must be re-established if the limb is avascular. A shunt should be considered if prolonged ischemia has occurred or is anticipated. If possible, vital structures such as vessels, nerves, tendons, and bones should be repaired primarily. Depending on the mechanisms of injury, the condition of the patient, and the options available, primary wound closure is preferred. If there is any doubt about the viability of the tissues that remain in the wound, the wound should be managed temporarily with the use of topical saline dressings or a negative pressure device, which can maintain a moist wound environment for 48 to 72 hours. A second-look procedure should be scheduled within 24 to 48 hours.
During the second procedure, definitive coverage should be performed. In rare cases (i.e., after crush, avulsion, burn, or electrical injuries), this “second look” may not allow for the adequate determination of the viability of the tissues. When this occurs, delayed closure is preferred so that sufficient debridement can be assured.
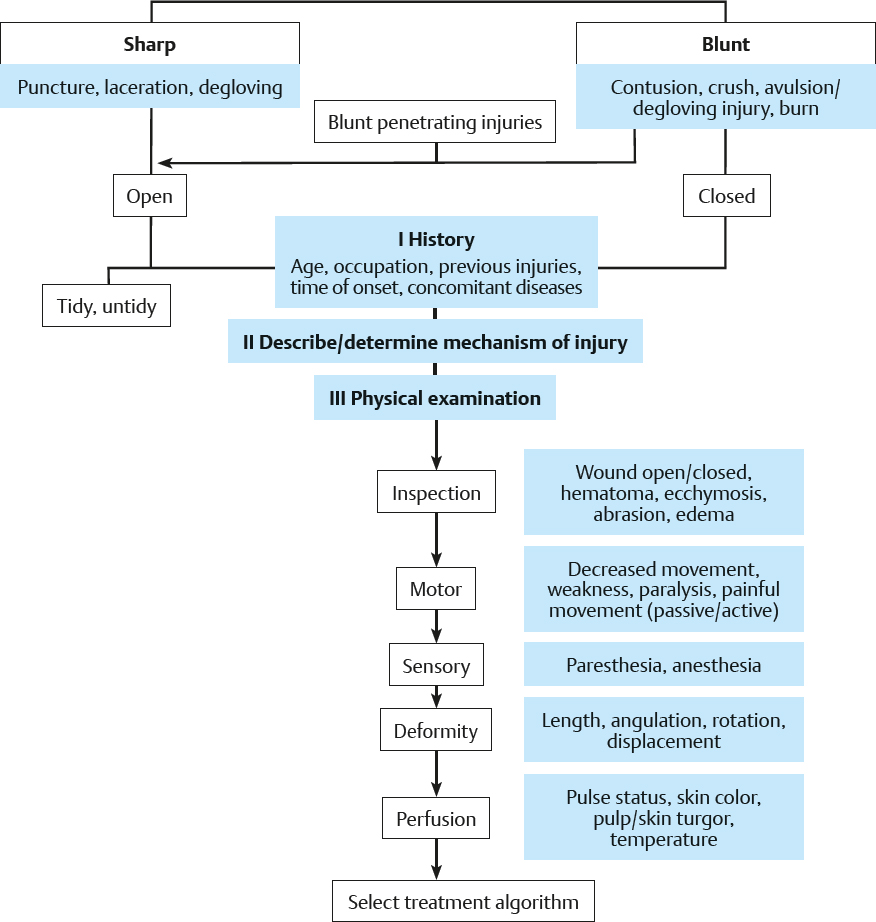
Patient Evaluation Algorithm