!DOCTYPE html>
18. Emotional Aspects of the Injection of Silicones with the Aim of Body Transformation
Keywords
AnxietyBody self-imageDepressionDysphoric feelingsEmotional aspectsFirst Silicone Awareness WeekIdeal bodyPatient-doctor relationshipPersonality disorderPsychosisSelf-imageThe human body is in the mind; it exists psychically. This means that in human experience, one’s own body exists subjectively, as a psychological phenomenon. We live our body, and the perception of it is determined by affective life, fantasy, and unconscious history. We construct the world in terms of our subjectivity, and the world we construct includes our body in relationship to the body of others. There is no human life without a body nor human body without psychological life.
All along different times and cultures, the body has been modified in its appearance and by means of dress. Clothing the body is not only a means of protection against weather conditions nor a supplement to make it more resistant to external climatic or environmental demands or against traumatisms. Even among peoples whose life takes place in nearly total nakedness, this is not complete: penis sheaths or feathers as ornaments are used at least (as occurs with New Guinea aborigines or the Zoé culture in Amazonia, just to name two examples). Clothes are always related to symbolisms, rituals, and cultural hierarchies; social conventions established in each time and place regarding dress determine modesty and beauty.
Fashion has an enormous impact and determines habits in our current occidental world. It is also a significant economical and industrial factor. It implies ways of carrying the body, ways of showing it or hiding it, highlighting certain volumes or anatomical shapes, attenuating or accentuating proportions, restricting or favoring movement, etc.
Since the first stages of psychological development, management of bodily functions through training is fundamental for socialization, and to exhibit or to hide the body is a central part of education for living together, in interaction with others. We are our body. This implies that the experience of the body becomes enigmatic and problematic and sets out questions on how the body is seen by others, on how it works internally. Aware of the gaze of others since the first moments after birth, we see ourselves reflected in their gaze, and we assess the degree of acceptance and reception depending on how we feel we are being seen.
The fact that there exist two evidently different anatomical configurations, male and female, surprises us prematurely and allows us to question ourselves about this difference since the solitude of infantile unconscious life to the most elaborate philosophical and cultural levels of cogitation (may we just mention Plato’s Symposium and the present-day debates and cultural studies on gender?).
Lesional and surgical interventions on the body to embellish it and for purpose of differentiation are known since antiquity. Scarification, deformation, tattoos, and diverse amputations are ancestrally practiced and have ornamental, liturgical, or magical aims. The first records of plastic surgery come from Egypt, Persia, and India and describe rhinoplasty, long centuries before the Christian era. Tastes, tendencies, and what is acceptable or not have changed throughout history according to existing conventions and ideals.
In the last decades due to technological advancements, which have changed the whole conception of the world and life, there has been a transformation of the experience of the body. New devices and techniques have allowed interventions and practices up to recently unfeasible and given place to an ideology centered in technology. A machine-like conception of the human organism has settled, even with the possibility of extensive prosthesis that amplify functional capabilities (cyborg-like).
Life has been manipulated since conception; gene editing and the artificial development of tissues and organs have endorsed the conception of mastering the body. Our body self-image is easily contrasted with an ideal body, deathless and damage-free. Over the last decades, technological advances in medicine together with extensive publicity that trivialize difficulties have led to a new conception of the body, where the owner can choose to accept or reject it. Progress in technology is implemented without previous thinking on the unforeseeable consequences to follow. Our own body thus turns out to be a device to be used.
Once the body is thought of as a machine, it may be replaced, tuned up, reassembled, and reconstituted following one’s own desires. I may have received the wrong body, as a result of some error in the assembly line. I have the fundamental right to ask for replacements of parts of it or to repudiate what I see, expecting different compensations. From this conception of the humane, medicine carries the burden of providing such compensations. Medical competences are not only relief of suffering, help to heal illness, or getting the sick body to work again. The physician becomes a provider of spare parts and a technician who must meet every others’ expectations and ideals regarding their bodies.
Thus, consultations to specialists in plastic surgery and aesthetic medicine have largely multiplied, but in a new modality of demand and consumerism, consumer demand and consumer satisfaction. Far from being consulted about ailing or limitations, the physician is forced to provide what is being demanded. Contrariwise, the doctor will be abandoned, seeking (and finding) the proper provider. It is no longer the case of health and illness; the issue is to obtain merchandise, the same as going to the supermarket or to a car dealer. So, interventions with drugs, substances, or physical procedures on the body are no longer considered medical therapeutics, except for their complexity or whenever the procedures are thought of as hazardous. The greater the ignorance, the smaller the perception of risks or greater the avoidance of due medical consideration.
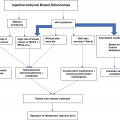
It is easy to imagine the day, soon, when it might be possible online to obtain a small surgical robot that performs simple surgeries at home, guided by an ad hoc algorithmic program driven by a software. The user now takes responsibility into his own hands, perhaps with some training, gives his consent, and undergoes the procedure. All in all, as proprietor of the body, he has the right to do with it whatever conforms to his wishes and illusions. There is not a great distance between the example just proposed and the injection of industrial silicone to change the shape of the body. Those who provide the silicone or inject it act in favor of the ideal and the desire of the person who requires it and is therefore considered an ally and even a benefactor. When complications arrive, the doctor is the bearer of bad news; he is the one who indicates surgeries against the initial expectations and who provokes suffering. Medical assistance demands decisions based on a way of thinking that is far from the usual habits of thought of the person who recklessly modified his/her body in search of an illusion of beauty, searching attraction and acceptance, and satisfaction with his/her self-image.
Anxiety and depression are frequent reactions to unwanted complications: pain, tumors, deformities, skin problems, and chronic systemic repercussion. The uncertainty caused by the symptoms (such as in any pathology) is perceived as threatening and provokes insecurity and incomprehension, resulting in anguish and the different manifestations of anxiety. The experience of loss and failure triggers depression. The person’s identity may be shaken by the unexpected pathologies that appear; that is, personal integrity may be upset beyond the failure of what was considered a glad solution. These manifestations are equivalent to those that happen during any illness or as a consequence of suffering undesired effects due to a surgery. They are not specific to silicone injection or silicones.
The greater the dissatisfaction with one’s own body, the less the capacity of integration of the personality. Dysphoric feelings are expressions of anxiety, a signal of internal conflict, insecurity, and inadequateness. In the small sample of patients, we assessed in our service during the first Silicone Awareness Week organized by Dr. Schenone in 2018, we verified that personality disorders were the most prevalent diagnosis. But not all of these disorders shared dysphoric symptoms. In fact, the rating of self-perceived quality of life according to VAS (Visual Analogue rating Scale of health-related quality of life) was high. The selection of patients was undoubtedly biased due to targeting of the announcements on certain sectors of the population.
It may be considered that when there is a marked certainty about the inadequateness of the body or about the alienation to one’s own body, there is a degree of psychotic functioning that may not be directly apparent or evident. Psychotic developments have always some anchoring in contextual reality, and social conventions may legitimate psychotic production or even favor it. Indiscriminate circulation of new implant techniques, tissue regeneration and modification, and sometimes as simple cosmetic practices encourage actions at one’s own initiative. External reality trivializes the intervention on the body or sets the basis for psychotic ideals of corporal transformation. In both cases, without psychotic functioning or determined by it, risks are minimized, and ignorance is reinforced, limiting access to reliable information.
It must be pointed out that society, fashion, and group tendencies end up legitimizing pathological ways of functioning: it does not matter what or how am I doing something but the immediate result. This leads to disdaining the information on deleterious effects of certain substances and confiding instead upon untrained members of one’s own social group who offer to provide an apparent solution to a physical condition considered defective.
Then, when a medical consultation renders necessary due to complications, it is perceived as a punishment and the physician perceived as a persecutor. As the removal of tissues affected by the injected substance or even more invasive interventions may be deemed necessary, hostility towards the physician increases. Then the professional may be left, in search of a more “benevolent” one, putting life at risk or abandoning all therapeutic efforts.
The complex emotional situation succinctly described in the previous lines makes clear the great difficulties and the various forms of interaction in the patient-doctor relationship in the case of persons who suffer complications due to injection of silicone (or of other substances, implants, or negligent aesthetic interventions). These patients constitute a great challenge, testing the physician’s experience and expertise.
The patients’ anxiety and depression may become a heavy load to deal with. Ambivalence, resentment, or open hostility towards the medical proposals may frequently constitute insurmountable hurdles. The physician should be wary of these difficulties so as not to respond with boredom, irritability, or reciprocal hostility. He shall have to appeal to his empathic capacity and tolerance, understanding the patient’s global predicament so as to offer the most adequate treatment. Complex difficulties must be taken as interesting challenges in order to be accepted by the patient and assimilated into his life as someone who genuinely works in his favor, not as those who greatly harmed him by answering to his aspirations based on ignorance.
Those who unscrupulously inject substances into people to transform their bodies are unaware of or far away from the fundamental medical dictum: primum non nocere.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


