CHAPTER 5 Arthroscopy of the Hip
Early diagnosis and minimally invasive treatment of hip disorders are playing an increasingly important role in current orthopedic practice. Although described in 1931 by Burman, clinical application of hip arthroscopy did not evolve until the 1980s, when Eriksson and colleagues1 described hip capsule distention and distraction forces necessary to allow adequate visualization of the femoral head and the acetabulum. Glick and associates2 later described lateral positioning, cannula placement, and anatomic landmarks.
In a study correlating radiographic findings with hip arthroscopy findings, McCarthy and Busconi3 showed that the most commonly overlooked cause of pain was acetabular labral lesions. Acetabular labral tears detected arthroscopically also correlated significantly with symptoms of anterior inguinal pain.
Intra-articular hip lesions are often missed by radiologic studies commonly performed to evaluate intractable hip pain, including plain radiographs, arthrography, bone scintigraphy, CT, and MRI. Plain radiographs may show calcified loose bodies or joint space narrowing in degenerative joint disease (DJD), but do not detect labral tears or more focal cartilage changes associated with the early stages of DJD. The addition of contrast agents such as gadolinium in conjunction with CT and MRI has been shown to increase the diagnostic yield principally in the detection of labral lesions.4
LABRAL TEARS
Labral tears represent the most common cause for mechanical hip symptoms. Acetabular labral lesions occur anteriorly in most reported series.5–10 Labral tears can be classified according to location, morphology, and associated articular changes. With respect to location, tears can be anterior, posterior, or superior (lateral). The etiology of labral tears is currently undergoing dynamic debate. A widely accepted theory is that torque and hyperextension forces applied to the weight-bearing portion of the acetabulum subject the anterior labrum to higher mechanical demands, making it more vulnerable to injury and wear.
These lesions occur in the anteromedial portion of the labrum (Fig. 5-1). Symptoms may be preceded by a traumatic event, such as a fall or twisting injury, or may have an insidious onset in patients who have sustained occult trauma or have intractable hip pain related to athletic participation. Often the inciting event is a pivoting maneuver during an athletic activity (e.g., tennis, karate, hockey, football, or soccer). Patients with minor trauma without dislocation almost invariably have anterior tears, which are accompanied by mechanical symptoms and intractable pain. Labral tears secondary to trauma are generally isolated to one particular region depending on the direction and extent of trauma. Physical examination findings can include any or all of the following: a positive McCarthy sign (with both hips fully flexed, the patient’s pain is reproduced by extending the affected hip, first in external rotation, then in internal rotation), inguinal pain with flexion, adduction and internal rotation of the hip, and anterior inguinal pain with ipsilateral resisted straight leg raising.6
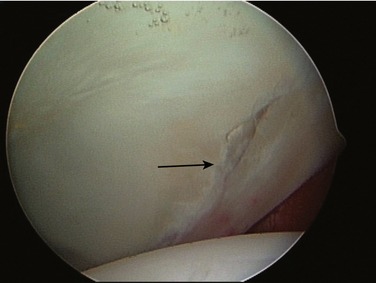
A current theory that has gained much attention focuses on congenital abnormalities of the acetabulum and proximal femur, which sometimes result in decreased anterior offset of the femoral head causing “cam”- or “pincer”-type impingement (or both).11,12 In these cases not only the etiology is different, but also the location of lesions. Labral lesions caused by bony impingement, although still found in the anterior quadrant, tend to occur anterolaterally (Fig. 5-2).

CHONDRAL LESIONS
Acetabular chondral lesions may occur in association with loose bodies, posterior dislocation, osteonecrosis, slipped capital femoral epiphysis, dysplasia, and degenerative arthritis; they are also frequently seen in association with labral tears. Chondral injuries are most frequently associated with a labral tear, they also are most often located in the anterior acetabulum. The severity of the chondral lesion is highly correlated with the surgical outcome; this severity can be graded according to Outerbridge’s criteria.13 Patients with fraying or a tear of the labrum often have chondral lesions, most of which are located in the same region of the acetabulum adjacent to the labral tear.14 The severity of the chondral lesions (Outerbridge grade III or IV) (Fig. 5-3) is greater in patients with labral tears or fraying than in patients with a normal labrum.

The most frequently observed chondral lesion is the watershed lesion (Fig. 5-4). This lesion consists of a labral tear with separation of the acetabular cartilage from the articular surface at the labral-cartilage junction. The watershed lesion, which occurs at the labral-chondral junction, may destabilize adjacent acetabular cartilage. When the damaged labral cartilage is subjected to repetitive loading conditions, joint fluid is pumped beneath acetabular chondral cartilage causing delamination of the articular cartilage. By this same mechanism, the fluid eventually burrows beneath subchondral bone to form a subchondral cyst. It is important to note that this cyst is the result and not the cause of the patient’s symptoms (Fig. 5-5). These cysts sometimes may be visualized on a plain radiograph in the absence of joint space narrowing or other degenerative changes, but are more frequently detected on MRI.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


