This article presents an introduction to economic outcomes for the plastic surgeon investigator. Types of economic outcomes are introduced and the matter of perspective is discussed. Examples from the plastic surgery literature are presented. The current and future importance of economic outcome measures is emphasized.
Key points
- •
Economic outcomes are gaining stature as health care funding dwindles.
- •
The complex mix of payers in the specialty of plastic surgery makes collecting economic outcomes more difficult, but also more important.
- •
When creating or assessing an analysis including economic outcomes, it is essential that the perspective is clearly stated.
- •
To maintain a position of national policy relevance, plastic surgeons must include economic outcomes in analyses.
- •
In today’s health care climate of scarce funding, it is prudent to include economic outcomes in comparative effective research whenever feasible.
In the 1950s and 1960s, as growing access to medical care led to concerns about increasing costs, research focus turned to the results of interventions. This new attention toward the end effects of treatment was dubbed the “outcomes movement” and was labeled the “third revolution in health care” by then-editor of the New England Journal of Medicine , Arnold Relman. Outcomes research strives to understand the results of interventions. These results are any patient experiences, including mortality, complications (or lack thereof), function, or quality of life, and can be reported by the provider, the patient, or by a third party. As the movement spread, reporting of outcomes became almost cursory. The increased prominence of outcomes led to what some call the fourth revolution in health care, namely, evidence-based medicine. Evidence-based medicine seeks to analyze and compare the outcomes, benefits, and risks of medical treatments, drugs, and devices to guide decision making by health care providers, consumers, and payers. This is hoped to reduce rapidly growing health care spending thought to be caused, partially, by the lack of evidence for the effectiveness of many costly, innovative treatments. Lack of evidence is not limited to new innovations, however; 85% of common medical treatments have not been rigorously validated.
In today’s health care marketplace, economic outcomes are increasingly becoming part of the assessment of medical interventions. Economic outcomes are indeed outcomes because they are a result of a care encounter, although they are not typically considered as such. The rate at which new surgical techniques are introduced in plastic surgery makes the field especially conducive to the analysis of economic outcomes. However, a systematic review of plastic surgery outcomes research from 1998 to 2004 found that only 3% of studies reported economic outcomes. Possible reasons for this include unfamiliarity of plastic surgery investigators with economic outcomes and that, for some procedures, costs are borne by patients. To maintain a position of impact on health care policy, plastic surgeons need to include economic outcomes in their research whenever feasible. The aim of this paper is to inform plastic surgeon investigators on the basics of economic outcomes and provide examples of their use in the plastic surgery literature.
What are economic outcomes?
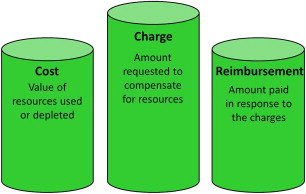
The most simple economic outcome is cost—the actual value of the resources consumed or depleted while providing a service. Costs can be divided into several categories. Direct costs are generally the items one first thinks of when considering costs: Supplies, medication, and personnel. Fixed direct costs are those that remain the same regardless of the number of times the service is provided. These items, such as facilities, administrative costs, and durable equipment, cost roughly the same amount to own irrespective of frequency of use. Variable costs, likewise, are reliant on the number of times a service is provided. For instance, labor is largely dependent on the availability of work. Combined with direct costs are indirect costs. These costs are more difficult to quantify and include items such as lost wages owing to time off of work or decreased work ability. Even more difficult, or nearly impossible, to calculate are intangible costs, a monetary representation of non-financial outcomes such as pain, suffering, and even negative effects on relationships. The final item in the calculation of total costs is opportunity costs. These costs represent the lost value when resources cannot be used in another manner. For instance, if an operating room is being used for a procedure that brings a hospital little income, it cannot be used for a more lucrative procedure. This may be less of an issue for plastic surgery, because the specialty’s hypothetical opportunity costs are low when compared with other surgical specialties. To obtain a complete picture of costs, it is important to include all of these elements.
Costs are not the only economic outcome. Charges may also be the outcome of interest. Charges are how much is billed for a service, which may not reflect the actual cost. Reimbursement, the amount received in exchange for a service, can be used as an outcome as well. In general, charges are higher than costs, owing to inclusion of profit and protection against uncompensated costs. Reimbursements vary from $0 to the full amount charged and may be set by a third party, as in the case of Center for Medicare and Medicaid Services (CMS) reimbursement rates. The tenuous relationship between these 3 economic outcome measures means that they are not interchangeable ( Fig. 1 ). It is important to know which one is being used when a study is assessed. Likewise, when performing a study it is equally important to specify which outcome is being used.
Whose perspective?
When using traditional outcomes measures, it is easy for all parties to come to a consensus on what constitutes a good outcome. Patients, providers, and third-party payers can all agree that reduced pain is positive. However, matters of finances are less clear. Whereas patients may experience better aesthetic outcomes after a more expensive intervention, if the provider is not recouping costs, it is not universally favorable. Therefore, it is important for researchers to be explicit about who is benefitting from the intervention under investigation. This is important information for readers of published studies because only studies performed from the same perspective can be compared.
The perspective taken depends on the research question being asked; there is no standard “best” perspective. Owing to the public nature of CMS reimbursement rates, assessing outcomes from a CMS perspective is relatively simple. Because other third-party payers base reimbursement rates on CMS rates, these figures can be extrapolated to third-party payers as a whole. With many plastic surgeons operating private practices, examining economic outcomes from the provider perspective can be enlightening, including specific outcomes, such as revenue (the amount earned) or profit (the amount earned after operating costs are subtracted). In the last decade, however, there has been a shift toward patient-rated outcomes; thus, there has been an increased interest in the economic ramifications of interventions on patients. This is in line with movements to empower patients and encourage their active role in health care. The patient perspective can be difficult to generalize. For procedures that are covered by third-party payers, patient costs can be negligible, placing more emphasis on indirect costs such as travel costs or lost wages, which are highly variable. The patient perspective is also the most likely of all perspectives to include intangible costs, which are nearly impossible to quantify. The societal perspective takes into account everyone who is impacted by an intervention, including individuals who are generally not considered, such as tax payers or coworkers who must work extra hours to cover for an ill employee. However, including all of these viewpoints can be exceedingly difficult; to truly represent the perspective of society, members of the general public should provide values.
Ideally, all costs that result from an encounter should be tallied, including cost savings if an intervention avoids a more expensive outcome, as well as difficult to calculate indirect, intangible, and opportunity costs ; however, it is impossible to include every item. For this reason, economic analyses are often based on a variety of assumptions, including estimated costs. Costs can be varied over a range of values to determine the robustness of the estimates to draw conclusions despite difficulty calculating exact costs.
Examples in Plastic Surgery Literature
Provider perspective
When considering the provider perspective, whether individual surgeon, practice, or institutional, it is important to consider operating costs in addition to revenue. Given the perceived low reimbursement rates for postmastectomy breast reconstruction, Alderman and colleagues sought to assess the impact of a variety of procedures on an academic plastic surgery practice and on the institution as a whole. Practice costs included physician salary, benefits, continuing medical education, malpractice insurance, and taxes, whereas institution costs were composed of fixed costs such as facility costs and variable costs such as nurse salaries and the costs of anesthesia. Also included were indirect costs, such as administrators’ salaries. Revenue was in the form of reimbursements, and profit was calculated by subtracting costs from revenue. This analysis illustrates the importance of distinguishing between charges and reimbursements. For both the institution and the practice, reimbursements were markedly less than charges. The institution received 56% of the amount billed, whereas the practice received only 32%. Despite this, overall an academic plastic surgery practice collects a profit of 27% for breast reconstruction, whereas the institution collects a 15% profit. To compare procedures, the authors calculated reimbursements by amount of time spent in the operating room. Delayed tissue expander plus implant reconstruction brought in the highest reimbursement/operating room hour, more than 5 times more than immediate transverse rectus abdominis myocutaneous flap reconstruction, which was reimbursed at the lowest rate.
Alderman and colleagues bring to light the issue of perspective, countering low physician and instruction reimbursement with evidence that patients prefer the aesthetic outcomes after transverse rectus abdominis myocutaneous flaps. Situations such as this are likely to only grow in number as our health care system attempts to balance financial constraints with an engaged public.
Third-party payer perspective versus patient perspective
Minimally invasive procedures may cost less, and may require less operating room time, often fewer staff, and generally shorter hospital stays. For these reasons, minimally invasive procedures are generally preferred by payers and patients alike. However, when hospital stays are shortened, there is often more home care involved and these costs may add up as well. Abbott and colleagues compared the costs with third-party payers as well as non-covered patient costs associated with 2 treatments for sagittal synostosis: Cranial vault remodeling, which is more invasive and requires a long hospital stay, and endoscopically assisted suturectomy, which is associated with shorter hospital stays, but requires the use of an orthotic device and numerous outpatient visits. Third-party payer costs included both hospital and physician costs. Hospital costs included costs that could be directly attributed to patients, such as supplies and medication. Overhead costs, such as building maintenance and administration, that cannot be attributed to a single patient were included using a formula to estimate the proportion of these items used. Physician costs were calculated on a departmental basis by determining a cost-to-charge ratio for each specialty involved. Non-covered patient costs were indirect costs incurred by patients (or in this case patients’ families), including wages loss for hospitalization and follow-up visits, gas and auto wear and tear associated with driving to the hospital and to appointments. These are, of course, estimates based on patient populations as a whole; naturally, individually costs vary widely.
The authors found that cranial vault remodeling costs almost twice as much as endoscopically assisted suturectomy ($55,121 vs $23,377). However, the costs to patients were significantly greater after endoscopically assisted suturectomy than after cranial vault remodeling ($3088 vs $2835, P <.001), owing primarily to cost associated with outpatient follow-up visits. This highlights the importance of considering the costs to all parties involved. Treatment that is less costly to the health care system may increase costs to individuals. Although the cost difference to patients is minimal in this example, in some cases it may render the “cheaper” option unaffordable.
Related posts:
 Patient-Reported Outcomes Instruments
Patient-Reported Outcomes Instruments
 The Outcomes Movement and Evidence-Based Medicine in Plastic Surgery
Development and Psychometric Evaluation of the FACE-Q Satisfaction with Appearance Scale
Measuring Outcomes in Craniofacial and Pediatric Plastic Surgery
Measuring Outcomes in Hand Surgery
Measuring Outcomes in Lower Limb Surgery
The Outcomes Movement and Evidence-Based Medicine in Plastic Surgery
Development and Psychometric Evaluation of the FACE-Q Satisfaction with Appearance Scale
Measuring Outcomes in Craniofacial and Pediatric Plastic Surgery
Measuring Outcomes in Hand Surgery
Measuring Outcomes in Lower Limb Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


