2
Anesthesia and Wound Closure
All wounds should be clean of foreign bodies and adequately irrigated (see Chapter 1). Hemostasis is achieved with pressure, silver nitrate, fibrin, Surgicel (Johnson & Johnson, New Brunswick, NJ), thrombin, or suture ligature (absorbable for small vessels and nonabsorbable for larger vessels) to prevent hematoma formation. Any devitalized tissue as well as jagged edges should be trimmed for optimal cosmesis.
Wounds can be closed with sutures, staples, skin tapes, or wound adhesives. Generally, wounds should be closed in layers using appropriate sutures and the epidermis reapproximated relatively tension free and everted if possible. Everted skin edges eventually flatten out and produce a level wound surface where the inverted skin edge persists to produce a valley-like scar.
In order to guarantee a successful wound closure a comfortable environment should be created for both the practitioner and patient. The use of analgesics, local anesthesia, and—at times—sedation are helpful adjunct in reducing patient anxiety. This will ultimately increase the likelihood of more precise closure.
 Anesthesia
Anesthesia
Local Anesthetics
Local anesthetics work by affecting the sodium (Na+) channels on afferent sensory nerves. Local anesthetics enter the cell membranes and reversibly binding to the Na channels, the cells are then unable to depolarize. Lidocaine is probably the most commonly used and accessible local anesthetic agent in the emergency room (ER).Epinephrine can be used along with lidocaine to decrease the amount of lidocaine needed, prolong the duration of the anesthetic, and decrease the amount of bleeding from the site (through vasoconstriction). The maximum safe dose for lidocaine is 4 mg/kg. With the addition of epinephrine (usually at 1:100,000 concentration), the maximum dose increases to 7 mg/kg.
A 1% solution of lidocaine is defined as
1 g/100 cc = 10 g/1000 cc = 10,000 mg/1000 cc = 10 mg/1 cc
Example Maximum dose of lidocaine with epinephrine in a 70-kg (154-lb)man
70 kg × max dose (7mg/kg) = 490 mg of lidocaine
490 mg × 1 cc/10 mg (concentration of 1% lidocaine) = 49 cc
of 1% lidocaine with epinephrine
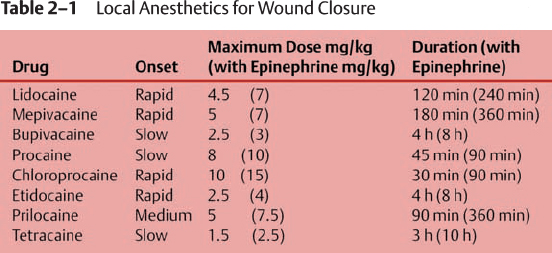
Epinephrine should not be used near end arteries, including the penis, digits, the nose, or stellate lacerations to avoid ischemia and necrosis. Wait 7 to 15 minutes for the epinephrine to become effective. Table 2–1 provides other local anesthetics that may be used with their maximum dosages and duration of action.
Once you have chosen your local anesthetic, it is useful to add bicarbonate to the solution, particularly when the patient is awake. The pH of local anesthetic solutions is generally buffered between 4 to 5 to prolong shelf life. Due to this acidity, patients often experience burning on injection. By adding a base to the local anesthetic, the action will also be accelerated because the higher pH favors the nonionized form of the anesthetic, which crosses the cell membrane more easily. The addition of 1 cc of a 1 mEq/mL solution of bicarbonate for every 9 cc of local anesthetic can alleviate this burning and improve patient comfort. Warming the anesthetic, using a 25-gauge needle or higher, and injecting by inserting the needle within the wound (instead of through the skin), helps in decreasing the pain felt by the patient on injection.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


