This article reviews Mohs micrographic surgery for basal cell carcinoma. Its evolution to the present day technique, indications, and limitations are discussed, along with future expectations for the procedure.
Mohs micrographic surgery in the management of basal cell carcinoma
Basal Cell Carcinoma
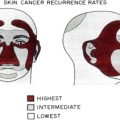
Basal cell carcinoma (BCC) makes up about 80% of all skin cancers, and it has been estimated that approximately 1 in 4 Americans will develop BCC during their lifetime. BCC is highly associated with ultraviolet radiation exposure, and as such, the most common locations for it to develop are the head and neck ( Box 1 ). Although BCCs are usually asymptomatic and only rarely metastasize, if left untreated, they can lead to significant functional and cosmetic morbidity ( Figs. 1 and 2 ).
- •
Eyelids
- •
Lips
- •
Ears
- •
Nose
- •
H-zone
- •
Genitalia
- •
Fingers and toes


In general, treatment of this slow-growing and rarely metastasizing type of skin cancer is simple and straightforward, particularly for lesions on the trunk and extremities. In these locations, techniques such as curettage (often in combination with electrodesiccation or cryosurgery) or simple surgical excision can provide high cure rates. However, treatment can be more challenging in cosmetically sensitive locations such as the head, neck, and genital area. In these regions, it is particularly crucial to both completely remove the neoplasm, thus limiting recurrence, and preserve function and appearance as much as possible. These requirements have led to the development of Mohs micrographic surgery (MMS) as the most widely accepted treatment of BCC in areas with the greatest demand for tissue preservation and those at greatest risk for recurrence.
MMS
As it is practiced today, MMS has evolved significantly from its first description as chemosurgery by Dr Frederic Mohs in 1941. Initially, his technique involved direct injections of zinc chloride solution into the tumor and surrounding area for in vivo tissue fixation. After 12 to 24 hours, the involved tissue was removed from an often bloodless field for microscopic examination. However, instead of traditional vertical sections, the tissue was oriented into tangential sections, which examined the entire peripheral and deep margins and led to cure rates approaching 99%.
Over time, Dr Mohs and others contributed to advancement in the field by introducing the removal of fresh tissue under local anesthesia for evaluation. In 1970, Dr Theodore Tromovitch presented the first series of patients using the fresh tissue technique. This series was followed by another supporting study by Tromovitch and Stegman in 1974. Both these studies illustrated success rates that were comparable to the previously described fixed tissue technique, opening the door to all of the potential benefits of using the fresh tissue technique without sacrificing the excellent outcomes that were achieved with the older method. These benefits included the following:
- 1.
Decreased pain for the patient. The previously used chemosurgical technique with in vivo tissue fixation was associated with significant presurgical and postsurgical patient discomfort, often requiring hospital admission for narcotic analgesia. This discomfort was caused by the significant pain and edema within and around the surgical wound from the chemical fixative.
- 2.
Increased efficiency for both the surgeon and the patient. Rapid freezing of the tissue could be used for microscopic evaluation within a matter of minutes instead of the slower zinc chloride fixation that took hours to complete.
- 3.
Vastly improved cosmetic outcomes and decreased wound healing time. Following complete eradication of the tumor with the fresh tissue technique, the surgeon was now able to immediately reconstruct and close the associated defect. With the former in vivo fixed tissue technique, a rim of devitalized tissue was created, which could not be repaired until it had sloughed spontaneously, often taking weeks. This delay in reconstruction resulted in allowing many wounds to heal by secondary intention, leading to much slower healing and, in some instances, poorer cosmetic outcomes for the patient.
Improvements in systems and equipment associated with the MMS procedure have continued to advance since the 1970s; nevertheless, the concept of complete margin control through tangential sections of excised tumor, as first reported by Dr Frederic Mohs, still prevails in the procedure as it is practiced today.
What makes MMS different from surgical excision with standard pathologic evaluation
Tumors treated by standard excision with vertical histologic sectioning are traditionally removed with margins large enough to have a statistically satisfactory high cure rate without recurrence (usually 3–4 mm for low-risk BCCs and larger margins for higher-risk tumors) ( Box 2 ). To achieve an acceptable rate of success, a significant amount of normal tissue has to be removed. However, when the Mohs technique is used, minimal margins can be obtained as the entire peripheral and deep margins of the lesion are examined histologically, removing the need for taking extra tissue to allow for a margin of error.
- •
BCC with poorly defined clinical margins ( Fig. 3 )

Fig. 3
Infiltrative BCC with poorly defined clinical margins on the posterior helix.
- •
Multiple BCCs associated with syndromes ( Fig. 4 )

Fig. 4
Multiple BCCs associated with basal cell nevus (Gorlin) syndrome.
- •
Large and deeply penetrating BCC ( Fig. 5 )

Fig. 5
Large and deeply penetrating BCC, which eroded into the trapezius muscle.
- •
Morphea-like, sclerotic, micronodular BCC ( Fig. 6 )

Fig. 6
Morphea-like, sclerotic BCC on the right medial cheek.
- •
Superficial multicentric BCC ( Fig. 7 )

Fig. 7
Ill-defined superficial multicentric BCC.
- •
Metatypical (basosquamous) BCC ( Fig. 8 )

Fig. 8
Metatypical (basosquamous) BCC.
- •
BCC arising within a scar ( Fig. 9 )

Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 Mohs Surgery for Squamous Cell Carcinoma
Mohs Surgery for Squamous Cell Carcinoma
 Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
 Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


