The treatment of diabetic foot ulceration is complex with multiple considerations often leading to limb amputation. This article presents the usefulness of a multidisciplinary approach along with an algorithm to manage and salvage diabetic foot ulcers from amputation. This algorithm is a step-by-step guide to manage the diabetic foot ulcer and can help one in the selection of patients for limb salvage reconstruction.
- •
A multidisciplinary approach is needed to initially control and treat multiple factors causing severe diabetic foot ulceration.
- •
Attention should be given to not only the wound but also the whole spectrum of care.
- •
The surgical steps of debridement, infection control, and vascular intervention are key steps to stabilize the wound and to prepare for a successful reconstruction.
- •
Reconstruction should provide a well-vascularized tissue to control infection, adequate contour for footwear, durability, and solid anchorage to resist shearing forces during gait.
Introduction
Chronic ulceration of the lower leg is a frequent condition, with a prevalence of 3% to 5% in the population older than 65 years. The incidence of ulceration is increasing because of the aging population and increased risk factors for atherosclerotic occlusion, such as smoking, obesity, and diabetes. Although most leg ulcers are caused by venous insufficiency (approximately 45%–60%), arterial insufficiency (10%–20%), diabetes (15%–25%), or combinations of these, the most debilitating of them is ulcers caused by diabetes.
According to the statistics given in the United States, approximately 3% to 4% of individuals with diabetes currently have foot ulcers or deep infections and 25% will develop foot ulcers sometime during their life. Their risk of lower leg amputation increases by a factor of 8 once an ulcer develops. It is estimated that the age-adjusted rate of lower extremity amputation in patients with diabetes is 15-fold that in individuals without diabetes. Intractable diabetic foot ulcers can bring not only decreased physical, emotional, and social functions but also huge economic impact to the patient. Furthermore, the 5-year mortality after major amputations may range from 39% to as high as 80%. Hence, salvage for diabetic foot ulcers remains important because it will reduce the economic burden and improve the quality of life.
Multidisciplinary approach
The spectrum of diabetic foot disease may vary from asymptomatic to critically ischemic limb with unavoidable amputation. The wide manifestation of symptoms is because of multifactor pathophysiology. The principal pathogenesis involves ischemia, neuropathy, and infection, and the addition of external trauma, peripheral edema, and foot deformity may further increase the risk for diabetic foot ulceration. These conditions may act alone or synergistically to result in Charcot deformities, Achilles tendon contractures, ulcerations, necrosis, and gangrene. One must consider these pathologic conditions and manage them in sequence to provide an efficient care for the foot.
Treatment must begin with strict control of blood glucose level and nutritional support while aggressively managing the wound and infection to achieve closure of the defect. In patients with ischemic limb, vascular bypass or angioplasty may play a vital role to enhance circulation allowing further reconstruction of soft tissue and bone.
The nurse specialist or coordinator helps to use the team recourses efficiently. After gathering general information about the patient and initial screening of the systemic and foot condition, the specialist would refer to endocrinologist, nutritionist, and proper departments for further treatment and evaluation. There are 4 categories for initial foot evaluation:
- 1.
Vascular
- 2.
Neuropathic
- 3.
Orthopedic
- 4.
Infectious wounds.
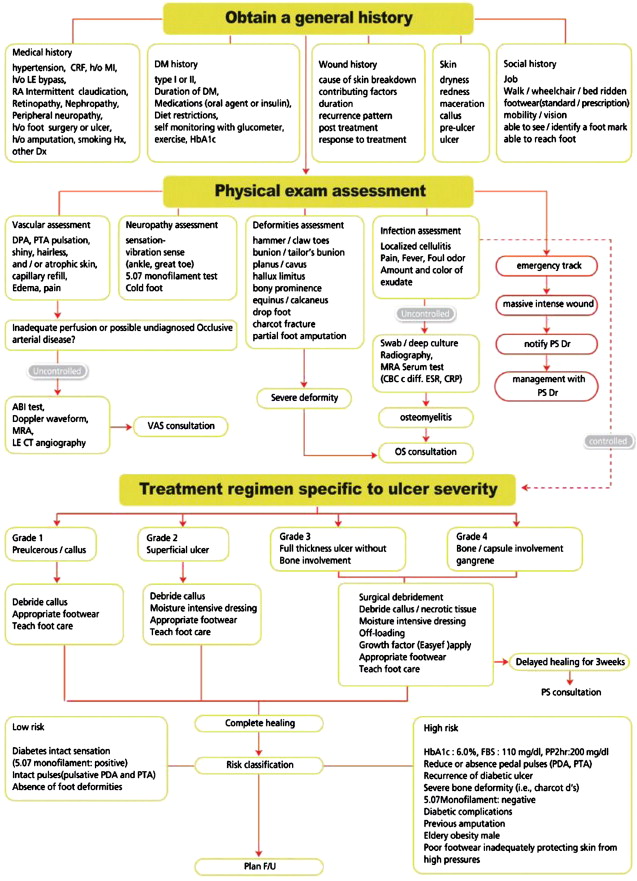
Multiple departments may be involved simultaneously to improve the patient’s foot condition. In cases of emergent wounds in the authors’ center, a plastic surgeon would be notified immediately for emergency debridement and further clinical decision. This is the first and also a major step to limit the spread of acute infection and to salvage of the diabetic foot. The coordinated approach is efficient because no time is wasted waiting for consultations, and it ensures the involvement of proper parties and integrates departments to work closely when undergoing challenging decisions and surgical treatment. Fig. 1 shows the multidisciplinary algorithm for primary screening and initial treatment of wounds.
With the introduction of a multidisciplinary approach, the trend of management has shifted from major amputation to limb salvage. By addressing the issues of perfusion, infection, wound treatment, off-loading, and bone surgery, the salvage rate is increased. Similar with other reports, the major amputation rate for diabetic foot in the authors’ center has reduced significantly after multidisciplinary approach and recently maintains to be about 3% to 4%. Although the indications for major amputation still exist and often are caused by multiple factors, such as
- •
Systemic sepsis
- •
Major tissue loss
- •
Significant comorbid factors
- •
Poor patient compliance
- •
Nonreconstructable peripheral vascular disease.
Multidisciplinary approach
The spectrum of diabetic foot disease may vary from asymptomatic to critically ischemic limb with unavoidable amputation. The wide manifestation of symptoms is because of multifactor pathophysiology. The principal pathogenesis involves ischemia, neuropathy, and infection, and the addition of external trauma, peripheral edema, and foot deformity may further increase the risk for diabetic foot ulceration. These conditions may act alone or synergistically to result in Charcot deformities, Achilles tendon contractures, ulcerations, necrosis, and gangrene. One must consider these pathologic conditions and manage them in sequence to provide an efficient care for the foot.
Treatment must begin with strict control of blood glucose level and nutritional support while aggressively managing the wound and infection to achieve closure of the defect. In patients with ischemic limb, vascular bypass or angioplasty may play a vital role to enhance circulation allowing further reconstruction of soft tissue and bone.
The nurse specialist or coordinator helps to use the team recourses efficiently. After gathering general information about the patient and initial screening of the systemic and foot condition, the specialist would refer to endocrinologist, nutritionist, and proper departments for further treatment and evaluation. There are 4 categories for initial foot evaluation:
- 1.
Vascular
- 2.
Neuropathic
- 3.
Orthopedic
- 4.
Infectious wounds.
Multiple departments may be involved simultaneously to improve the patient’s foot condition. In cases of emergent wounds in the authors’ center, a plastic surgeon would be notified immediately for emergency debridement and further clinical decision. This is the first and also a major step to limit the spread of acute infection and to salvage of the diabetic foot. The coordinated approach is efficient because no time is wasted waiting for consultations, and it ensures the involvement of proper parties and integrates departments to work closely when undergoing challenging decisions and surgical treatment. Fig. 1 shows the multidisciplinary algorithm for primary screening and initial treatment of wounds.
With the introduction of a multidisciplinary approach, the trend of management has shifted from major amputation to limb salvage. By addressing the issues of perfusion, infection, wound treatment, off-loading, and bone surgery, the salvage rate is increased. Similar with other reports, the major amputation rate for diabetic foot in the authors’ center has reduced significantly after multidisciplinary approach and recently maintains to be about 3% to 4%. Although the indications for major amputation still exist and often are caused by multiple factors, such as
- •
Systemic sepsis
- •
Major tissue loss
- •
Significant comorbid factors
- •
Poor patient compliance
- •
Nonreconstructable peripheral vascular disease.
Spectrum of care
When considering diabetic foot for reconstruction, there are multiple issues to be addressed. These issues can be effectively approached through a multidisciplinary approach.
- •
The first step is to control the systemic aspect of diabetes. Malnutrition, chronic renal disease, and hypertension have to be addressed properly and treatment schedules set before and after surgery, especially hemodialysis and perioperative blood glucose control.
- •
While the systemic condition of the patient is being optimized, specific attention can be directed to the foot ulcer. Depending on the general condition, peripheral vascular status, bone pathology, wound depth, location, duration, involvement of chronic osteomyelitis, and patient motivation, wounds can be treated with debridement and other related surgical procedures.
- •
Another important issue is the vascular pathology of the patient. The vascular surgery consultation is essential when the patient is symptomatic with ischemic pain or a nonhealing ulcer. Neuropathic ulcers require debridement of nonviable or infected tissue, combined with local wound care and off-loading.
If the condition of the diabetic wound is not improved by such procedures or aggressive wound care, foot salvage procedures can be considered. A robust predictor of healing is 53% change in the wound area of diabetic foot ulcers. The authors’ monitor the change in wound size and depth, and when wound healing is stalled despite good standard of care, such as off-loading, infection control, edema control, and advanced dressings, additional treatment with hyperbaric oxygen, cell therapy, growth factor treatment, and negative pressure wound therapy is considered. Depending on the complexity of the wound, some of these secondary modalities are used primarily as well. The progress of wound healing is closely monitored, and stalled healing, despite these multimodal therapies, may become one of the indicators for reconstruction. Fig. 2 shows the spectrum of care for diabetic foot ulcers from general care to reconstruction or amputation.
Role of microsurgery
Until recently, reconstruction with microsurgical techniques has been under debate. This was due to the incorrect concept, first attributed to Goldenberg and colleagues in 1959, that patients with diabetes have an increased incidence of small vessel disease that results in foot ulcers. Particularly, it was thought that patients with diabetes have arteriolar occlusive disease, which can cause ischemic lesions. The investigators studied amputation specimens from patients with gangrene and concluded that patients with diabetes have endothelial hypertrophy and proliferation in the smaller arteries, with complete occlusion of the lumen in several cases.
But subsequent studies failed to demonstrate increased arteriolar occlusive disease or endothelial proliferation. A thickening of the capillary basement membrane has been documented but not capillary narrowing or occlusion. This same study showed that diabetics often have atherosclerotic occlusion of the tibial arteries, but the occlusive disease occurs mainly in the leg, so that the arterial system in the foot is less involved. Based on these studies, limb salvage from diabetic foot using microsurgical approach showed similar success comparable to that from non-diabetic patients. Meta-analysis of a systematic review of free tissue transfer in 528 patients with diabetes in 18 studies showed that flap survival was 92% and limb salvage rate was 83.4% over a 28-month average follow-up period. This study indicates that free tissue transfer in the management of nontraumatic lower extremity wounds in patients with diabetes may avoid amputations. Free flaps and microsurgery technique now play an important role in the salvage of the limb from chronic ulcerations. This review presents a surgical algorithm for limb salvage focused on the microsurgical reconstruction ( Fig. 3 ).
The use of this algorithm gives one a general guideline on important steps:
Pearls
- 1.
Good standard of care, including debridement, dressing, off-loading, and edema control
- 2.
Vascular intervention
- 3.
Reconstruction with local and free flaps
Pitfalls
One must understand that this is not an absolute step-by-step approach but rather a back and forth approach. Decision for amputation should not be made easily and all efforts should be taken, including exploration for recipient vessels, to ensure that there is no alternative to amputation.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


