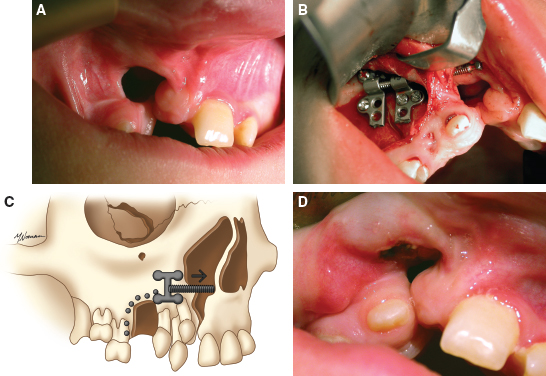
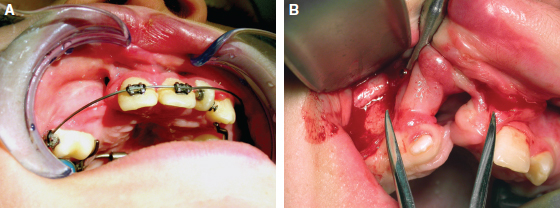
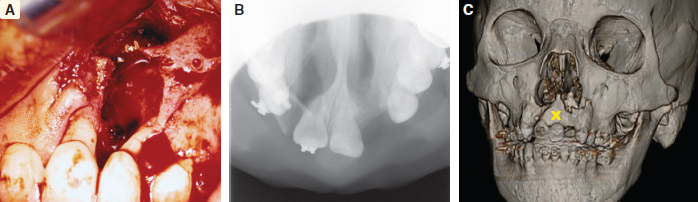
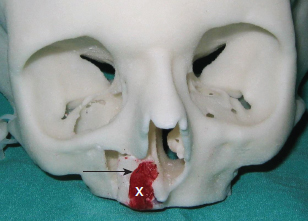
70 ○ Patient selection for alveolar transport distraction osteogenesis and its ultimate success involve patient motivation, parent and patient commitment to the procedure and postoperative course, and excellent oral hygiene. ○ Preoperative planning using three-dimensional imaging and models to execute the projected movements is vital to confirm ultimate segment positioning and stability. ○ Local tissue health and integrity with enough attached gingiva for final “docking” of the distracted segment and bone grafting of the defect is necessary before initiating distraction. ○ The reconstruction team consists of a surgeon, an orthodontist, and a restorative dentist (prosthodontist) who agree on the plan and timing for distraction. ○ Simultaneous anterior maxilla and piriform distraction can be achieved through distraction of a larger dentoalveolar segment, thus augmenting these regions, with or without grafting. Management of the alveolar cleft defect (ACD) has often been a challenging aspect of the comprehensive management of patients with orofacial clefts. The ACD results from intentional delay in treatment or failed attempts at repair during primary cleft lip or palate surgery. Typically, ACDs result in a collapsed, disunited arch with unsupported lip, nasal, and dental elements. The concomitant oronasal fistula (ONF) contributes to sinonasal inflammation, drainage, and periodontitis. Therefore repair of the osseous defect and closure of the fistula are considered important aspects of complete cleft management. Fig. 70-1 A, Right unilateral cleft with wide, disparate alveolar segments. B, Right unilateral cleft with deficient soft tissue and a wide bony defect. Repair of the ACD has a long history in cleft care. The goals for adequate treatment include1,2: Attempts at ACD closure by performing gingivoperiosteoplasty at lip repair have been met with varying results, oftentimes necessitating future formal repair with bone grafts. The timing of ACD repair also has been controversial. Primary osteoplasty, with placement of autogenous bone at or near the time of initial lip repair, has been both condemned and championed. Many results have been less than ideal, again with the need for further bony augmentation of the alveolar segment.3–5 Secondary osteoplasty of the ACD is considered the treatment of choice for many cleft teams, principally because it is predictable and achievable, satisfying the goals of repair as stated previously. Early secondary osteoplasty, as advanced by Boyne and Sands6 as well as others, attempts to graft the ACD before eruption of the permanent incisors.7,8 Delayed secondary osteoplasty has been shown to be effective and predictable for most children when it is performed before the complete root formation of the adult canine tooth, around 10 to 12 years of age.9,10 Delayed secondary osteoplasty is usually performed in conjunction with preparatory orthodontics and after some orthopedic manipulation to optimally position the cleft segment. However, a significant number of patients experience failed bone graft procedures, have very wide defects with collapsed cleft segments, or have significantly scarred ACDs with questionable soft tissue covering, all of which make further attempts at bone grafting rather dubious and unsatisfying. This is aptly termed recalcitrant ACD (Fig. 70-1) and is especially challenging in particular circumstances: a lack of healthy unscarred mucogingival tissue lining the ACD, deficient alveolar bone height and width against which the graft must be placed, older patients with decreased bony healing potential, and the presence of compromised dentition or prostheses with little bone support.11 Recently, distraction osteogenesis (DO) has been developed for application in the craniofacial region. Smaller regional areas of the facial skeleton have been distracted to optimize functional and aesthetic units for future orthopedic or orthodontic correction, grafting procedures, or prosthodontic rehabilitation. In 1905, Codivilla12 initially described the concept of DO to lengthen a femur, correcting a limb length discrepancy. In the 1950s, this application was more widely applied to orthopedic limb lengthening. The landmark research into this technique by Ilizarov13 looked at the development of distraction techniques, devices, and rates on bone formation. He developed the technique on canine long bones and then applied the protocol to human patients, pioneering many of the concepts of DO, including recommendations on latency, distraction rate, and distraction rhythm. In 1992, McCarthy14 applied DO to the unilateral mandibular deficiency found in hemifacial microsomia. He lengthened the affected mandible in children using an external fixation device, which allowed calibrated distraction between external pins holders. At the completion of the distraction phase, the mandibles were stabilized for a mean period of 9 weeks. DO of the midface region has been performed by devices categorized as internal or external devices. Several maxillary DO devices have been used to advance the maxilla through either various osteotomies at the LeFort levels or segmentation of the maxilla.15 These procedures are discussed in Chapters 73 and 74. To achieve maxillary arch widening, Bell and Epker16 used a DO technique of rapid palatal expansion with a tooth-borne expander, increasing the transverse dimension of the maxilla after osteotomies had been performed. Guerrero and Bell17 further developed these techniques, using incremental expansions of 1 mm every other day, up to a total of 10 mm, to obtain significant transverse expansion of the arch. This concept was applied to the alveolar segment by Chin and Toth,18 who looked at regenerating alveolar bone after trauma using an internal distraction device with a transmucosal activation screw. Block and Baughman19 further applied DO to the vertically deficient alveolar segment, increasing bone height before implant placement. Simultaneous secondary bone grafting was performed in many of these cases after final alveolar segment distraction. Use of alveolar distraction is now widespread for preprosthetic manipulation before rehabilitation.20 Cleft alveolar distraction has been performed and studied by Liou et al,21 who used various osteotomies and appliances to approximate cleft segments, narrow the ACD, and improve arch dimension. Others also have applied DO to correct various cleft-related problems, such as a narrow or collapsed maxillary arch and a wide ACD with insufficient soft tissue, and to prevent bone grafting an ACD.22–25 Distraction has become an important tool in the management of particularly difficult or recalcitrant ACDs, discussed later in detail. Several indications for alveolar transport DO exist. A very wide ACD may preclude a bone graft if soft tissue and alveolar bone are deficient (see Fig. 70-1). A patient who has had a previous failed bone graft may be considered for transport DO to achieve the goals of standard alveolar cleft surgery (Fig. 70-2). Older patients who have not been treated for their ACD may be candidates for transport DO to narrow the defect and thus require minimal secondary grafting, improving the success for prosthetic rehabilitation. Fig. 70-2 A, A failed primary osteoplasty with a persistent defect. The failed bone graft was done at age 1. The patient has a fistula and insufficient osseous support for dental structures. B, Partial osteoplasty of a bilateral cleft defect with failure of the graft on the patient’s right. C, A patient with a partial osteoplasty on the left and complete failure on the right side. Alveolar cleft defects are, by nature, multidimensional, and have different defect combinations including the anteroposterior, horizontal, and vertical dimensions. Depending on the specific defect, transport DO may be considered for definitive treatment or to address the largest dimensional deficiency, thereby improving the quality and quantity of alveolar bone. This will allow for an easier and minimal secondary bone graft procedure. This process is particularly applicable when treating vertical alveolar deficiency. Vertical alveolar DO may be considered to increase alveolar bone height after grafting and when planning placement of an implant for later prosthetic rehabilitation. Several contraindications to alveolar cleft DO exist. A surgeon should be wary of initiating alveolar DO for patients with clefts who have not been compliant in various aspects of their treatment. DO is a very labor-intensive process, requiring a great deal of cooperation from the patient and caregivers; therefore education is crucial before initiating treatment. Patients with active dental issues should have these addressed, with consideration given to optimizing oral health before surgery. Periapical disease should be eliminated to prevent infection during the distraction period. In patients younger than 10 years of age, the potential exists for damage to developing teeth and impairing the eruption pattern in the area of distraction. This needs to be thoroughly discussed with the patient and family beforehand. Indirectly associated with compliance are the patient’s general health and condition of the local tissues. If any concern exists related to these areas, avoiding this mechanically technical procedure and the potential subsequent complications of tissue breakdown and loss of the device may be prudent. Children who have poorly controlled chronic asthma or allergies, resulting in nasal obstruction and patterns of mouth breathing that increase oral tissue inflammation, may be prone to intraoral tissue compromise and breakdown. For these reasons, optimal intraoral health should be maintained through primary care and pediatric dental management. Once these concerns have been satisfied, then plans for distraction can be undertaken. Fig. 70-3 An acrylic model of a right unilateral cleft defect (X) demonstrating planned distraction of the alveolar segment (arrow). As with all aspects of comprehensive cleft care, management of the ACD benefits from a team approach. Preparing the patient and family for the various aspects of therapy is important before initiating alveolar transport DO. In addition, coordination of the team involved in perioperative management is essential. The patient’s pediatric dentist should be involved well before transport DO is considered to optimize oral health before surgery. Any carious lesions should be addressed and periodontal disease eradicated before the patient is assessed for surgery. Questionable or nonvital teeth should be treated before DO is begun to eliminate the possibility of infection jeopardizing the distraction process. Orthodontic consultation and management is important to address dental and arch discrepancies before the repair of the ACD, whether by conventional bone grafting or by movement of the alveolar bone using distraction. The arch may require expansion before formal repair of the alveolar cleft, and the orthodontist must be involved in the planning and management during distraction. Finishing dental and arch alignment is the orthodontist’s responsibility. Prosthodontic management of the patient may be required postoperatively for the replacement of missing teeth. This may involve the placement of crowns or bridges, or the surgical placement of implants if bone stock is adequate. The patient must appreciate that grafted bone must be completely mature before implants can be placed, a period of approximately 3 months.26 Consultation with the prosthodontist is important to evaluate the arch space and bone height that will be needed for prosthetic rehabilitation. Three-dimensional acrylic models (Fig. 70-3) are a great help to the treating team, patient, and caregivers who will be involved in the distraction process. Precise placement and activation of the device can be achieved and demonstrated. The caregivers need to be instructed in the cleansing and hygiene of the activation rod. Perioperative antibacterial mouth rinses (oral chlorhexidine) and oral antibiotics should be carefully reviewed and dispensed. Pain medications and dietary instructions will need to be adjusted based on individual patient needs. Most children will have adequate analgesia with ibuprofen, which may be administered before or after each distraction event, as indicated. It is important to instruct the patient and caregivers about the objectives of DO and to create realistic expectations for what can be achieved. Instructions for care may have to be given in stages and over several preoperative appointments to establish a thorough understanding before and during treatment. The patient and family need to appreciate that DO may not be able to completely correct the anatomic deficits. Further surgery, in a second stage, will be required to remove the distractor; at that time, the defect can be simultaneously augmented with additional bone graft if necessary. As in many ACD reconstructions, final and acceptable soft tissue coverage may be required in a separate procedure to provide adequate attached gingiva around the teeth and implants. Vital to the success of any intraoral surgical procedure, particularly around the dentition and any abnormal anatomy, is optimal soft tissue composition and health. Loss or limitation of healthy keratinized tissue around the dentition may compromise the general integrity of the periodontium, leading to further bone loss or predictable bony surgery in the future. Studies have demonstrated that patients with cleft lip or palate have more periodontal compromise in the cleft defect area, including loss of a zone of healthy keratinized tissue.27,28 Although loose (unattached) mucosa may serve as a temporary healing or covering measure, such as labiobuccal mucosa grafts placed during primary or early secondary osteoplasty, this does not serve well for periodontal integrity in the long term. If plans are made for segmental osteotomy or distraction of a cleft segment, healthy abutting transposed attached (keratinized) tissue, both palatally and labiobuccally, is preferable. Soft tissue inadequacies such as these are seen especially in older cleft patients who have undergone multiple procedures, resulting in compromised soft tissue in and around the alveolar cleft defect and dentition.29 If a lack of healthy soft tissue is determined during the evaluation process, then plans should be made to graft the area to provide this tissue. Autologous graft from the palate (preferred) or acellular dermis graft can be placed in the immediate defect area and periodontium.30 After a period of maturation, variably 8 to 12 weeks, when keratinization is complete and inflammation resolved, subsequent bony surgery can be undertaken. When juxtapositioning the alveolar segments during final distraction, flap elevation and coverage of the bone graft should be easier and final closure more predictable with appropriately healthy mucogingiva. Unilateral ACDs are more common and often have problems with significant asymmetry and excessive defect width. Although skilled interceptive orthodontics can often successfully align and position the lesser segment and narrow the defect width, occasionally the poorly positioned cleft segment will remain, with suboptimal soft tissue that would compromise, and potentially prohibit, orthodontic treatment. A typical case is illustrated in Fig. 70-4. This patient had a long history of cleft surgical procedures, as well as two phases of orthodontics. The ACD was still poorly positioned with extensively scarred soft tissue; the radiographs verified a significant bony defect width between the segments. This situation is difficult to correct with conventional orthodontic preparation and alveolar bone grafting; therefore distraction of the cleft segment, to narrow the defect by approximating the alveolar segments, will increase the success of a smaller bone graft. A single vector alveolar distractor was placed on the buccal aspect of the lesser segment after vertical osteotomy between the bicuspids and horizontal osteotomy, approximately 7 to 8 mm above the level of the root apices. The activating rod is oriented in a favorable position under the lip for easy access. Postdistraction photos demonstrate an alveolus more favorably positioned for bone grafting. Many alveolar distractors offer various distracting lengths (10 to 20 mm) and multiple options for plate and screw placement (Fig. 70-5). The device should be contoured to the alveolar surface so that activation will move the segment in the desired direction. Some distractors allow for orientation of the activation rod from 0 degrees (coaxial to the distractor) to 30 degrees to allow favorable rod positioning and access for daily activation. Minimal activation should be performed during the surgical procedure to prevent undue tension on the overlying soft tissue, which may tear and compromise vascularity. Two or three millimeters of activation, to confirm complete mobility of the osteotomized segment, will suffice at the time of distractor placement.
Alveolar Transport Distraction Osteogenesis
Bruce B. Horswell, Nicholas J.V. Hogg
KEY POINTS
HISTORY OF DISTRACTION OSTEOGENESIS
Principles of Distraction Osteogenesis
Maxillofacial Application
PREPARATION FOR ALVEOLAR DISTRACTION OSTEOGENESIS
Patient Selection and Indications
Contraindications
Patient Preparation
Soft Tissue Preparation
CASE EXAMPLES
Unilateral Cleft Defect
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine