Fig. 27.1
Urticarial lesions (By permission of B Cohen and CU Lehmann, DermAtlas, Johns Hopkins University, 2000–2007)
Clinical Features of Urticaria
Clinically, urticarial lesions are intensely pruritic and can appear anywhere on the body, typically appearing quickly and lasting 1–24 h [8]. Unlike other pruritic skin diseases such as atopic dermatitis, patients with urticaria find relief from rubbing the skin versus scratching, making excoriated skin a less common finding in CSU [9]. Lesions can vary in size and can be confluent (see Fig. 27.1). The swelling observed with urticaria results from the movement of plasma from small blood vessels into adjacent connective tissue [4]. Angioedema often coexists with urticaria, and develops from a deeper, swelling of the dermis, subcutaneous, and submucosal tissues. Angioedema is described as painful or burning in quality, and is rarely pruritic [10]. It frequently involves mucous membranes with common locations being the face, lips, tongue, pharynx, and extremities (see Fig. 27.2) [9]. In contrast, urticaria, both acute and chronic, rarely involves mucosal surfaces [10]. Angioedema typically has a slower resolution time than hives, often greater than 24 h and larger areas may take longer to resolve [9, 10].
Fig. 27.2
Angioedema (By permission of B Cohen and CU Lehmann, DermAtlas, Johns Hopkins University, 2000–2007)
History and Physical Exam
In diagnosing either acute or chronic urticaria, a good history is the most critical element (see Fig. 27.3). It is important to assess the time of onset of hives, as some patients may experience diurnal variation, as well as the temporal association with certain environmental exposures or stressors. The most important aspect of history-taking is to identify the inducing agent for the patient’s urticaria and/or angioedema. This involves questions regarding recent use of medications, including antibiotics, nonsteroidal anti-inflammatory agents, and aspirin. A history of food ingested shortly prior to symptom occurrence, recent changes in environment, and possible insect stings should also be sought.
Fig. 27.3
Diagnosis algorithm for urticaria
Patients should provide a description of lesions including elements such as shape, size, distribution, color, pigmentation, and the quality of pain or itch. Urticarial lesions are typically pruritic and usually demonstrate complete resolution without skin pigment changes. A clinician must also assess for the presence of angioedema in association with urticaria. In patients with isolated angioedema without urticaria, family history is critical to assess for hereditary angioedema (HAE), an autosomal dominant condition resulting from a defect in C1 esterase inhibitor function [10].
Additional questions should include recent infections, thyroid disease symptoms, surgical history of implantable devices, and for females, the relationship of hives to their menstrual cycle or pregnancy. Further evaluation of exposures, including patient’s work, may assist in understanding the timing or exacerbation of lesions. It is also important to evaluate how the patient is coping and what therapeutics, including nonprescription medications and dietary regimens, are being used and if they are providing any relief.
Along with the detailed history, the physical exam in a patient with urticaria can be helpful in excluding other disorders. It is important to do a complete exam as well as assess for dermatographism, wheals brought out by stroking of the skin (see Fig. 27.4). The size, distribution, and color of lesions should be noted. Wheals are characteristically pink or red due to histamine-induced dilatation of vessels in the skin while vasculitic lesions have a darker red or purple appearance resulting from vascular damage and leakage [6]. Urticarial lesions can be easily blanched. The physician should also inspect mucous membranes for the presence of angioedema (see Fig. 27.2). Patients should also be assessed for thyroid gland abnormalities on physical exam. Physical urticarias may require additional maneuvers, such as an ice-cube test to evaluate cold urticaria, and should be tailored to the suspected type of urticaria (see Fig. 27.5 and Table 27.1) [1]. No specific laboratory testing is needed for all patients with urticaria and should be dependent on the subtype of urticaria: acute, chronic idiopathic/spontaneous, or physical [11].

Fig. 27.4
Dermatographism (By permission of B Cohen and CU Lehmann, DermAtlas, Johns Hopkins University, 2000–2007)
Fig. 27.5
Ice-cube test for cold urticaria (By permission the Department of Dermatology, University of Iowa College of Medicine)
Table 27.1
Classification of physical urticaria
Type | % of all urticaria | Pathogenesis | Features | Reaction times | Provocation test | Differences on biopsy | Treatment |
|---|---|---|---|---|---|---|---|
Dermatographic | 7–10 % | Unknown, but elevated plasma histamine levels and positive passive transfer experiments, indicate an IgE-mediated process. | Mechanical shearing forces lead to lesions. Koebner’s phenomenon, a wheal and flare reaction at pressure sites (e.g. waistband), is present. Higher frequency in young adults. | (1) Immediate – within 2–5 min; lasting 30 min (2) Intermediate – within 30 min to 2 h; lasting 3–9 h (3) Late onset (rare) – within 4–6 h; lasting 24–48 h | Stroke forearm or back with tongue blade | Scant leukocytic infiltrate in upper dermis. | Nonsedating H1 blocker. |
Delayed pressure | 3–5 % | Unknown | Constant application of pressure to skin results in erythema and superficial and deep swelling. Pressure areas commonly affected. Male predominance. | Within 3–12 h; lasting up to 48 h | Application of weight to one area for minimum 10 min | Infiltrate typically located in mid- to lower dermis. Neutrophils may be seen in lower dermis. | Nonsedating H1 blocker. Short course of corticosteroids, leukotriene antagonists may also be used. |
Vibratory | Rare | Unknown, but elevated histamine levels and mast cell degranulation reported following application of stimuli. Familial cases have autosomal dominant inheritance. | Occurs after vibratory stimuli (e.g. lawn mowing or motorcycling). | Within minutes; lasting up to 24 h | Challenge with vibratory stimuli (e.g. vortex mixer) for 5 min | Avoidance of trigger. | |
Familial cold | Gene alteration at CIAS1 on chromosome 1q.44. Autosomal dominant inheritance. | Immediate type characterized by burning papules or macules and systemic symptoms such as arthralgias and fever. Delayed type follows cold exposure. | Delayed occurs within 9–18 h of cold exposure, lasting 2–3 days. | (1) Immediate – Polymorphonuclear infiltrates. (2) Delayed – Mononuclear infiltrates. | |||
Cold contact | 3–5 % | IgE-mediated histamine release with IgM and IgG antibodies reported. | Occurs with skin cold exposure. May have angioedema. Rare cases of anaphylaxis after total body exposure to cold. | Within 2–5 min as skin re-warms. | Ice cube placement to area for 10–20 min | Loose lymphocytic and leukocytic infiltrates. Platelet infiltrates and vascular changes may also be present. | Nonsedating H1 blocker. Leukotriene antagonist may be added. |
Heat contact | Unknown, but complement system is afffected. | Occurs at sites of heat application. Divided into immediate nonfamilial and delayed familial. | (1) Immediate – within 5 min; up to 1 h (2) Delayed – within 6–18 h; lasting 12–24 h | Local contact with hot water or object | Avoidance of trigger. | ||
Solar | Rare | Unknown, but thought to be IgE-mediated with increased serum histamine levels, mast cell and eosinophil degranulation, and photoallergen production. Secondary solar urticaria is characterized by a porphyrin metabolism abnormality leading to complement activation. | Induced by sunlight or indoor lighting exposure (wavelengths 280–760 nm). Most common in third and fourth decades of life, commonly affecting young adults. | Within 2–3 min; lasting 3–4 h | Expose to UV light | Avoidance of sun exposure and skin protection. Nonsedating H1 blocker. | |
Cholinergic | 2–7 % | Unknown, but acetylcholine, released by exercise, can release histamine. Elevated histamine and eosinophil and neutrophil chemotactic factors reported. | Due to a rise in core body temperature. Usually start on face and neck, then spreading. The pruritic wheals are small (1–5 mm) with “fried egg” appearance. More common in young adults. | Within minutes; lasting less than 1 h | Physical activity (e.g. running in place for 5 min) | Loose lymphocytic and leukocytic infiltrates in upper dermis. | Nonsedating H1 blocker. Increase dose if necessary. In addition, danazol can be used. |
Aquagenic | Rare | Unknown, but a proposed mechanism is that water induces formation of histamine-releasing substances. | Contact with water induces small hives similar to those seen in cholinergic urticaria. More common in young adults. | Within 2 min; lasting up to 1 h | Apply water compress for 30 min | Mast cell degranulation noted in challenged skin. | Avoidance of trigger. |
Contact | May be IgE-mediated. | Inciting triggers are plants, foods, drugs, and chemicals. | Within minutes; lasting less than a few hours. | Avoidance of trigger. | |||
Adrenergic | Unknown | Pin-sized wheals elicited by stress. | Within minutes; lasting less than 1 h | Propanolol |
Acute Urticaria
Acute urticaria is classified as hives of less than 6 weeks duration and accounts for up to 56 % of cases of urticaria [12]. Lesions are short-lived, lasting less than 24 h but can return [12]. Clinically, acute urticaria cannot be distinguished from chronic urticaria by physical exam alone. No routine laboratory testing should be done unless used to identify the trigger, such as in suspected food or drug reactions.
Acute urticaria can be classified as allergic (IgE-mediated) or nonallergic. IgE-mediated urticaria may occur in allergic responses to foods, insect stings, and drugs. Non-IgE mediated urticaria may occur in response to a “pseudoallergen” like aspirin, or result from other immunologic responses as seen with blood transfusions, serum sickness, and febrile illnesses [7].
Urticaria related to an IgE-mediated food allergy should occur within 30 min to 2 h following exposure. Testing for food allergies is appropriate in acute urticaria if the patient’s history reveals urticaria associated with other symptoms such as nausea or vomiting, however food allergies are not a common cause of acute urticaria in adults. In children, food allergy plays a larger role in acute urticaria, such as with milk, egg, soy, peanuts, and wheat [13].
Drugs can also be responsible for acute urticaria, through either IgE or non-IgE mediated processes. Drugs have been implicated as a cause of acute urticaria in 9.2–27 % of cases [12]. Penicillin is an example of an allergen, which can elicit urticaria through an IgE-dependent mechanism, while acetyl salicylic acid (aspirin) is a frequent non-IgE mediated stimulus for histamine release [12]. ACE inhibitors have also been implicated as triggers for angioedema through effects on the bradykinin pathway [10].
Viral infections are the most common reason for acute urticaria with onset of hives typically occurring a few days after the start of viral symptoms. The coexistence of acute urticaria and upper respiratory infections reported between 28 and 63.4 % [13–16]. Surprisingly, no identifiable trigger is found in 30–50 % of cases of acute urticaria [12].
Chronic Urticaria
Chronic urticaria by definition is wheals occurring at least 2 days per week of at least 6 weeks duration [17]. In contrast to acute urticaria, chronic urticaria is unlikely to be the result of IgE-mediated allergic reactions [18, 19]. Chronic urticaria can be divided into two subtypes: chronic idiopathic/spontaneous urticaria and physical urticaria. Chronic spontaneous urticaria (CSU) usually lacks an identifiable and consistent trigger, whereas physical urticaria is categorized into subtypes based on the specific trigger(s) which directly elicit hives within minutes. Lesions in physical urticaria generally do not last longer than a few hours, while CSU lesions typically are present for at least 6–8 h [4, 9, 17]. Some crossover exists between CSU and physical urticarias with 40 % of CSU patients displaying dermatographism [20].
Physical Urticaria
Physical urticaria is defined by the ability of a physical stimulus to reproducibly elicit urticarial lesions and accounts for 20–35 % of all cases of chronic urticaria [4]. Physical urticaria can be further divided into many subtypes depending on the physical stimulus (Table 27.1), and more than one subtype can exist simultaneously in one individual [17]. Evaluation of physical urticaria is strongly guided by the patient’s history and provocative testing.
Mechanical shearing forces, such as rubbing or scratching the skin, are the catalyst for dermatographic urticaria, the most frequent type of physical urticaria, where lesions arise a few minutes following application of the trigger [2, 7]. Features of physical urticarias can be common in the general population with dermatographism reported in approximately 2–5 % of subjects with no history of chronic urticaria [21]. Delayed pressure urticaria and angioedema result after vertical pressure is applied to the skin with lesions, often painful, appearing several hours after application and persisting for up to 48 h; this subtype of urticaria predominantly affects the palms, soles, buttocks, and back and has a male predominance [7, 22]. Vibratory urticaria is instigated by vibratory forces, is quite rare, and can be described as familial with autosomal dominant inheritance or may occur in sporadic pattern [21, 23].
Familial cold urticaria is an autosomal dominant disease mainly affecting young adults and is due to gene alteration CIAS1 at chromosome 1q.44. This gene locus is also involved in Muckle-Wells syndrome and autosomal dominant periodic fever syndrome, both are diseases that demonstrate cold-sensitivity [24, 25]. Cold contact urticaria, which occurs after direct contact of skin to a cold object or air, also occurs predominantly in women, younger adults, and cold climates. This subtype can be idiopathic or can be incited by bacterial or viral infections [22]. Heat contact urticaria is rare and results after the skin directly comes in contact with a hot object or warm air [21, 22]. Ultra violet light is the trigger for solar urticaria, an IgE-dependent subtype that occurs at wavelengths of 280–760 nm and more commonly affects females and young adults [21, 22].
Cholinergic urticaria is aggravated by a rise in body temperature and thus is triggered by exercise, bathing, emotions, and less with alcohol or spicy food consumption [21, 22]. Cholinergic urticaria typically involves young adults and is characterized by small, pin-sized wheals (1–5 mm diameter), sometimes with a white halo, that last for less than an hour. The symptoms of cholinergic urticaria can be so mild that an estimated 80 % of people with this urticarial subtype do not seek medical advice [7, 22]. Cholinergic urticaria should be distinguished from exercise-induced anaphylaxis which involves the development of systemic symptoms [21]. Adrenergic urticaria is also described as pin-sized wheals but unlike cholinergic urticaria, it is elicited by stress and can by treated with propanolol [21, 22]. Aquagenic urticaria, which is elicited by any exposure to water regardless of its temperature, mimics cholinergic urticaria in the appearance of its lesions, has a female predominance and more often affects young adults [21, 22].
Contact urticaria can be IgE-mediated or non-IgE-mediated, with the inciting triggers ranging from plants such as grass, foods like peanut, drugs, cosmetics, chemicals, and textiles. Contact urticaria has a short-lived duration like cholinergic and adrenergic urticarial subtypes, occurring within minutes of exposure, and resolving within a few hours [21]. Systemic symptoms can be present with contact urticaria, especially if IgE-mediated [22].
Chronic Spontaneous Urticaria
CSU accounts for approximately 80 % of all cases of chronic urticaria [11]. CSU is episodic and persistent in nature with typical disease duration of 3–5 years [26]. One prospective study of CSU subjects demonstrated that at 6 months, 94 % of patients were still active, 75 % at 12 months, 52 % at 24 months, 43 % at 36 months, and 14 % at 5 years [3]. Likewise, 18.5 %, 54 %, and 67.7 % of children were in remission at 1, 3, and 5 years, respectively, after the onset of symptoms [27]. Disease duration was directly correlated to the presence of severe disease, angioedema, and the presence of anti-thyroid antibodies [3]. Angioedema coexists with urticaria in approximately 40–50 % of CSU patients [26, 28]. The most common and bothersome symptom for patients with CSU is pruritus, which frequently adversely affects their sleep. Fatigue and gastrointestinal symptoms have been previously described with exacerbations, however respiratory complaints and arthralgia also noted [9, 29].
CSU can be a socially and financially disabling disease with an impact on quality of life, comparable to that of coronary heart disease [30]. One study of 170 chronic urticaria patients reported individuals with CSU alone experience a moderate impairment in their quality of life as measured by the Dermatology Life Quality Index (DLQI), while those with CSU and angioedema and/or delayed pressure features had significantly greater quality of life impairment [31]. Compared to other debilitating dermatological diseases, the quality of life impairment in chronic urticaria is similar to patients with severe atopic dermatitis and worse than patients with psoriasis, acne, and vitiligo [31]. Part of the frustration patients experience results from the lack of an identifiable trigger for urticarial exacerbations, leading to an unpredictable disease. CSU also carries an economic burden for patients with multiple medications, medical evaluations, work absence, and use of the emergency department [32, 33].
Aspirin and nonsteroidal anti-inflammatory agents (NSAIDs) can substantially aggravate urticaria and angioedema in CSU subjects via inhibition of prostaglandin synthesis. Selective cyclooxygenase-2 (COX-2) inhibitors lead to less symptoms than aspirin and traditional NSAIDs and provide an alternative choice for analgesics in CSU patients [34]. One study of chronic urticaria patients challenged with aspirin demonstrated that approximately 20 % of CSU subjects had a reaction, while those with physical urticaria were unaffected [35]. Patient history of suspected aspirin sensitivity correlates very well with reactions during aspirin challenges, as one study found that 92 % of patients with a history of reaction reacted during an aspirin challenge [36]. Patients should be advised that aspirin and traditional NSAIDs have the potential to exacerbate their disease, and should be informed that salicylates may be an occult ingredient in medications or supplements. Studies to assess the role of salicylates in foods demonstrated inconclusive results, and “low salicylate” diets are not generally recommended [11].
There is a higher prevalence of thyroid disease in CSU than in the general population. Hashimoto’s thyroiditis and, less commonly, Graves’ disease are the only reported systemic diseases with a correlation to CSU [37–40]. It has been reported that 27 % of CSU subjects have thyroid autoantibodies, nearly twice the rate observed in the normal population. Typically, the majority of those with thyroid autoantibodies are euthyroid and some may be hypothyroid, but it is rare for these individuals to be hyperthyroid [40–42]. Currently, these autoantibodies are not thought to be pathogenic in urticarial [43] but lend support to an autoimmune basis for a subset of CSU [44]. Studies of thyroid hormone replacement in patients with concomitant CSU and thyroid autoantibodies have yielded mixed results [43, 45]. The current recommendation is to screen patients for underlying thyroid disease and to treat any underlying thyroid disease, but no clear evidence exists for the use of thyroid hormone in euthyroid patients who present thyroid autoantibodies.
Histology
The classic wheal observed in both acute and chronic urticaria represents dermal edema with dilatation of postcapillary venules and lymphatic vessels (see new Fig. 27.6a, b) [46]. In biopsies, the leukocyte infiltrate is characteristically perivascular and classically consists of lymphocytes, neutrophils, macrophages, basophils, and occasionally eosinophils (see Fig. 27.6a, b) [47, 48]. Degranulated mast cells are also noted in urticarial lesions [48]. Histologically, CSU shares lesional features with acute urticaria consisting of a lymphocytic-predominant perivascular infiltrate. Occasionally, neutrophils are seen within capillary or post-capillary venule walls, but unlike the neutrophilic infiltrate seen in urticarial vasculitis, there is no evidence of vascular damage, nuclear debris, or red cell extravasation (Fig. 27.6b, c) [1]. The presence of intradermal CD3+, CD4+, CD8+, and CD25+ T-cells, as well as eosinophils, neutrophils, basophils, and macrophages is significantly higher in CSU skin lesions as compared to skin of nonatopic individuals [48]. A survey of basophil numbers in the skin biopsies from 24 skin diseases revealed that CSU had among the highest numbers of infiltrating basophils [49].
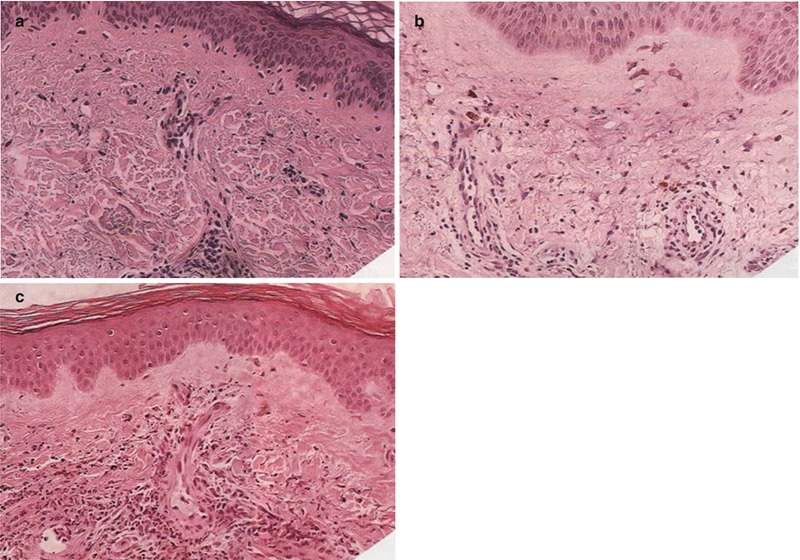
Fig. 27.6
Biopsy of urticarial lesion. (a) Representative of acute urticaria with dermal edema and a perivascular mononuclear infiltrate. (b) Chronic urticaria is may also have infiltration of neutrophils and/or eosinophils without evidence of vasculitis. (c) Urticarial vasculitis is shown with a large perivascular infiltration of neutrophils, and even some neutrophilic damage (By permission of Fireman and Savin [212])
Although the cellular infiltrate of CSU resembles that seen in allergen-induced late phase skin biopsies, the cytokine profile in CSU is TH1 and TH2 with higher expression of IFN-γ, as well as IL-4 and IL-5 in the skin [48]. By immunohistochemistry, TNF-α and IL-3 protein expression are increased in acute and chronic urticarial lesions [50]. TNF-α is a cytokine produced by epithelial cells, leukocytes, and mast cells [51, 52]. TNF-α can induce mast cell mediator release and increase endothelial adhesion molecule expression, thus an increase of this cytokine in urticaria may contribute to the leukocyte infiltrate observed [51, 53, 54]. IL-3 is a cytokine produced by mast cells, T-cells, monocytes, and granulocytes, and can increase expression of the endothelial adhesion molecule P-selectin [55–59]. P-selectin expression is elevated in both the skin and serum of chronic urticaria patients [60]. Two endothelial adhesion molecules, integrins ELAM-1 and ICAM-1, were upregulated in acute and chronic urticarial lesions [61]. The persistent expression of ELAM-1 and ICAM-1 in lesions older than 6 h may help to explain the long duration of urticarial wheals [61].
Pathophysiology of Urticaria
Whereas the pathophysiology of allergic urticaria supports a specific allergen interacting with IgE bound on skin mast cells, chronic urticarias do not appear to involve IgE binding to allergen [4]. The pathophysiology of both physical urticaria and CSU is unknown. Although mast cell degranulation is a clear component in some subtypes of physical urticaria (dermatographic, cholinergic, cold, and solar urticaria), serum IgE may also play a role as demonstrated by passive transfer experiments [9, 22, 42]. An acute rise in serum histamine and PGD2 levels has been observed in cold urticaria following cold exposure [62]. In CSU, there is also evidence for mast cell degranulation observed on skin biopsies [48]. Mast cell number appears to be similar in nonlesional and lesional CSU skin and normal skin, using tryptase and chymase staining [63]. Although mast cell number is not altered, increased mast cell releasability has been demonstrated in patients with CSU with active disease, which resolves with disease remission, suggesting that the mast cell alteration is reversible [64]. Cultured peripheral blood mast cells from CSU patients have been found to have higher levels of spontaneous histamine release compared to healthy controls [65]. In contrast, another study found higher levels of total tryptase (a reflection of the body burden of mast cells) in the sera of chronic urticaria patients compared to controls, but no difference was found in mature tryptase levels (reflects mast cell degranulation) [66].
There has been accumulating evidence that basophils play a role in CSU [67]. Basophils have been reported in both lesional and nonlesional CSU skin using BB1 staining [48, 49, 68]. Blood basopenia is a feature of active CSU disease, and the reduction in basophil number correlates inversely with disease severity [69, 70]. As seen with allergen late-phase reactions, basophils that have migrated to the skin may play a role in duration as well as magnitude of urticarial lesions [71]. Select basophil surface markers correlate to basophil activation and have been measured in CSU, in particular, CD63, CD69, and CD203c [72–75]. CD63 is a member of the transmembrane-4 superfamily is rapidly mobilized onto the basophil surface by IL-3, allergen, anti-IgE and other stimuli of degranulation while CD69 is slowly induced following IL-3 stimulation [72, 76]. CD203c, also known as ectonucleotide pyrophosphatase, is unique to basophils, mast cells, and their progenitors and is mobilized by allergen, anti-IgE, and IL-3 [77–81]. CSU subjects demonstrate enhanced basophil surface expression of CD63, CD69, and CD203c when compared to non-allergic controls [49, 75].
Furthermore, CSU basophils demonstrated a decreased functional response to IgE receptor stimulation but not to other stimuli [67, 82–85]. Early studies showed that histamine release mediated via the basophil high affinity IgE receptor, FcεRI, was diminished in subjects with CSU versus controls [84, 85]. This finding is paradoxical since anti-histamines are used to treat CSU, and pruritus, the predominant symptom in CSU, is histamine-dependent. A later study has shown that basophils in CSU have altered FcεRI-mediated histamine release and have found two patterns of histamine release within subjects with active CSU disease [83]. Approximately 50 % of subjects with CSU tested were found to be “responders,” releasing greater than 10 % of cellular histamine content when triggered with a polyclonal anti-IgE stimulus, and 50 % were “nonresponders”, releasing less than 10 % of cellular histamine content [83]. Also, these two basophil phenotypes appear to be stable over time as subjects maintain active disease, but this altered basophil function improves with disease remission [84, 86].
In a subset of CSU referred to as “autoimmune urticaria,” histamine-releasing autoantibodies have been reported and hypothesized to be pathogenic, although this remains controversial [44, 87–92]. These IgG autoantibodies are thought to activate mast cells and basophils via complement and act by C5a to potentiate histamine release [93]. These autoantibodies are detected in 30–40 % of patients with CSU, and the majority of these autoantibodies are directed against the alpha subunit of the high affinity IgE receptor, FcεRI, while the remainder directly target IgE [29, 89]. In favor of autoimmune mechanisms in CSU is the increased incidence of thyroid autoantibodies, specifically anti-microsomal and anti-thyroglobulin, as well as reports of higher frequencies of certain HLA class II alleles (DR4, DQ8) in CSU patients [37, 38, 40, 41, 94]. The autoantibody theory is also supported by the observation that autologous serum injected into a CSU patient’s skin can result in a wheal-and-flare response [95, 96]. However, a recent study demonstrated that healthy controls and patients with allergic rhinitis can also have a positive ASST, raising doubt about the usefulness of the ASST in the diagnosis of urticaria [11, 97, 98].
Since the presence of an ASST response alone does not prove that autoantibodies are present, further studies were done and demonstrated that sera from ASST-positive CSU subjects also had histamine-releasing activity (HRA) from healthy donor basophils [89, 99]. A large study found that 40 % of CSU subjects’ sera exhibit HRA when performed in vitro on donor basophils [88]. Although HRA is reported to indicate the presence of autoantibodies, the presence of HRA and the presence of autoantibodies by Western blotting in CSU subjects do not agree [100, 101]. The presence of serum HRA had no effect on the character of the leukocyte infiltrates of new (<4 h) or established (>12 h) skin lesions even though autoantibody presence has been previously linked to increased disease severity [48, 101, 102]. In addition, serum HRA has been demonstrated in healthy patients’ sera, and there is no correlation between HRA and CSU basophil FcεRI function [83, 103].
Another issue with the autoantibody hypothesis is that anti- FcεRIα autoantibodies are also found at a similar frequency in other autoimmune diseases like systemic lupus erythematous (SLE) and dermatomyositis as well as in normal subjects [104]. Similar frequencies of positive results have been found between CSU and SLE patients using a commercial test which measures the ability of a patient’s serum to trigger histamine release from donor basophils [105]. This lack of diagnostic specificity of the HRA assay raises concern about its usefulness in determining disease pathogenesis in CSU patients [103]. Also, anaphylaxis is rarely seen in CSU, which is a skin-limited disease, but would be expected to occur more often if autoantibodies directed against basophils and mast cells IgE receptor are present.
Laboratory Evaluation
In most cases of urticaria, history and physical examination are sufficient for diagnosis [6], and a thorough history may identify potential triggers such as medications. Patients with chronic urticaria who are resistant to conventional therapies or experience atypical lesion features (i.e., hyperpigmentation, bruising, prolonged duration) may need further evaluation to exclude secondary causes for hives. Laboratory testing should be limited because previous studies have shown extensive testing provides low yield [11, 106]. Patients who have symptoms or a family history of thyroid disease would warrant thyroid screening by measuring thyroid stimulating hormone and possibly thyroid autoantibodies.
For physical urticarias, patients are unlikely to benefit from further laboratory testing [107–109]. The physical exam can assist substantially in defining the type of physical urticaria that is present based on provocative tests (see Table 27.1). Patients with significant angioedema without urticaria should have complement levels checked along with C1 inhibitor testing (functional and quantitative levels) to screen for hereditary and acquired angioedema due to C1 esterase inhibitor deficiency which would result in low complement C4 levels [10].
Infections have been implicated in urticaria. As previously mentioned, viral infections, especially viral upper respiratory infections are a common cause of acute urticaria. A study in a Japan, which has a high prevalence of hepatitis C, demonstrated that this infection may manifest with chronic urticarial lesions, but further work in areas with lower prevalence has not supported this finding [110, 111]. It is recommended that individuals with risk factors for infectious hepatitis should have the appropriate testing. In recent years, Helicobacter pylori has been implicated to CSU but controlled studies have not been able to establish this link [112–115]. Parasitic infections are a rare cause of urticaria that should be investigated by stool examination for ova and parasites. Bacterial cultures are rarely necessitated as bacterial infections are not a common cause of urticaria [116].
Allergy testing may be of limited use in acute urticaria. Serum specific IgE testing (ImmunoCAP) or skin testing may be beneficial when a Type-I hypersensitivity reaction is strongly suspected. Skin testing is often difficult to perform in chronic urticaria patients due to the high prevalence of dermatographism and delayed pressure features in this group as well as their dependence on anti-histamines. ImmunoCAP testing is not affected by medications. A careful history can help to identify which allergens to test. Extensive food or inhalant allergy testing should not be performed blindly in patients with chronic urticaria as this does not improve patient outcomes and is not a cost-effective approach [11].
Another skin test used in the past to define autoimmune urticaria is the autologous skin serum test (ASST). Since the presence or absence of the ASST or autoantibodies does not alter treatment options in patients, the ASST should not be used as a diagnostic tool for chronic urticaria [7, 11]. Newer basophil-based assays to check for serum histamine releasing activity (HRA) also lack specificity and validation for clinical use [103, 105, 117, 118].
Other Conditions Associated with Urticarial Lesions
Urticarial vasculitis (UV) must be excluded in patients with chronic urticaria unresponsive to conventional therapy. UV is a Type-III hypersensitivity reaction mediated by antigen-antibody complexes deposited on vascular endothelium, and may be precipitated by infections, medications or neoplasms [119]. The duration of UV lesions is characteristically greater than 24 h and may be painful and purpuric, leaving residual skin changes [120]. These patients may also complain of systemic symptoms and have laboratory findings consistent with an inflammatory process, such as an elevated ESR or C-reactive protein or low complement levels [120]. To rule out urticarial vasculitis, the definitive test is a skin biopsy. The features of urticarial vasculitis on biopsy are leukocytoclasia, extravasation of red blood cells, fibrin deposition, leukocyte invasion of the vascular endothelium, and endothelial edema, of which the latter three features may also be observed in chronic urticaria (see Fig. 27.6) [1, 120].
There are other diseases associated with urticarial lesions, and patients presenting with appropriate symptoms should be evaluated for these disorders. Urticaria pigmentosa (UP), a subtype of mastocytosis, may mimic urticarial lesions with the exception that these are pigmented and typically longer-lasting lesions than those in urticaria. These lesions typically urticate with scratching (Darier’s sign), however, the diagnosis must be confirmed by biopsy and histology in each case [121, 122]. UP is often limited in children, as there is generally a spontaneous regression of the condition by puberty [123]. Adult mastocytosis, however, is an aggressive disease, and all adults with UP should have a total tryptase level measured and undergo a bone marrow biopsy [121].
Bullous pemphigoid (BP) is an autoimmune blistering skin disease which, in its early stages, may also present with urticarial lesions. The primary lesions of BP result from IgG autoantibodies are directed primarily against the BP 230 and BP 180 antigens, which are components of the hemidesmosome adhesion complex and allow the basal cells of the epidermis to adhere to the basement membrane. BP primarily affects older patients, and should be considered in urticaria develops in elderly individuals [120].
Subacute cutaneous lupus erythematosus (SCLE) can present with urticarial-like lesions which can be mistaken for CSU. SCLE is characterized by nonscaring lesions that typically burn more than they itch. These lesions tend to fluctuate in appearance and occur predominantly on sun-exposed areas of the body, often hours to days following significant sun exposure [120].
The presence of systemic symptoms along with urticaria should raise concern for additional conditions. Schnitzler’s syndrome is associated with recurrent urticarial lesions and dermatographism, fever, arthralgia, bone pain, lymphadenopathy, a high ESR, and IgM gammopathy. Patients with Schnitzler’s syndrome generally have a pale rose or red eruption consisting of macules papules, and plaques which tend to occur in crops, last <24 h, and are usually not significantly pruritic [124]. Angioedema is not a common is not feature of this condition. There is a delay in diagnosis (usually 5 years or longer) because most patients are instead labeled as having antihistamine-unresponsive CSU, and patients with these symptoms warrant a serum protein electrophoresis [120].
Sweet’s syndrome (acute febrile neutrophilic dermatosis) was first described in 1964 by Robert Sweet [125]. It is characterized by fever, neutrophilia (with blood polymorphonuclear leukocyte level greater than 10,000/mm3), and painful, erythematous papules or plaques (dense dermal neutrophilic infiltrate) on the extremities, face, and neck [125]. Classic Sweet syndrome is associated with infection of the respiratory or gastrointestinal tract, or may occur after vaccination. There is also a paraneoplastic variant of Sweet syndrome which is most commonly associated with lymphoproliferative disorders, and occasionally associated with solid malignant tumors [126].
Also presenting with fever and urticaria are serum sickness (SS), serum sickness–like reactions (SSLR), and urticaria multiforme. Both SS and SSLR present with fever, rash and arthritis 7–21 days after exposure to the offending antigen, which is most often a medication. It is critical that a medication history be elicited from these patients, and that suspected medication be promptly discontinued. Unlike classic SS, SSLR does not have detectable circulating immune complexes or hypocomplementemia, and its pathogenesis remains poorly understood. Urticaria multiforme primarily affects children, and involves urticarial plaques with a hemorrhagic pattern which appear 1–3 days following an acute viral illness [119].
Treatment
Acute Urticaria
For acute urticaria the most important step is to eliminate the trigger if identified. Patients can use antihistamines to help with symptom alleviation until resolution of the episode. Approximately 44–91 % of all urticaria patients treated with H1-antagonists found a benefit [127, 128]. Typically, non-sedating H1-antagonists are utilized although classic sedating H1-antagonists, such as diphenhydramine or hydroxyzine, may be used. The major risk associated with administration of first-generation H1-antagonists is somnolence [12]. For severe cases of acute urticaria, a short course of systemic corticosteroids may provide more prompt control [12]. One study reported that acute urticaria exacerbations lasted only 3 days in approximately 94 % of studied patients compared to only 66 % of patients not receiving steroids [129]. Topical steroids play no role in the treatment of urticaria since application would involve a large area of skin with minimal benefit [7].
Chronic Urticaria
The treatment of CSU is a greater challenge than that of acute and physical urticarias. The physician should explain to the patient the natural history of CSU and the lack of a cause as this may lessen patient frustration. Patients should avoid triggers, but these are rarely identified in CSU. Avoidance of certain potential triggers such as aspirin, nonsteroidal anti-inflammatory drugs, ACE inhibitors, and codeine-containing products that can directly stimulate skin mast cells is also recommended [7].
Second–generation antihistamines are first-line therapy for chronic urticaria [130]. H1-antagonists are used to control the intense pruritus associated with the CSU. One study reported that 94 % of patients with CSU had some itch relief with use of H1-antagonists, with the majority on the sedating type [131]. In patients with CU who do not respond adequately to second-generation antihistamines at FDA-approved doses, doses can be provided at higher than licensed doses, often with additional therapeutic benefit [130]. Similarly, the treatment of physical urticaria involves second-generation antihistamines and avoidance of triggers [132–137]. Some past studies in CSU patients demonstrated an improvement in dermatographism and pruritus with the simultaneous use of an H1-antagonist and H2-antagonist versus a H1-antagonist alone. Doxepin, a tricyclic antidepressant with some H1- and H2-receptor antagonist properties, may be useful for nighttime itch and has been shown to be more effective than diphenhydramine in the treatment of CSU [138]. Doxepin should not be used with MAO inhibitors due to a risk for Long QT Syndrome [7]. However, approximately 50 % of chronic urticaria patients do not respond to antihistamines and require additional agents to achieve symptom control [139, 140].
Success with leukotriene receptor antagonists has been reported for physical urticaria of the cold-induced and delayed pressure types, aspirin-sensitive urticaria, and food-induced acute urticaria [141–143]. However, there is conflicting results regarding the efficacy of leukotriene receptor antagonists in CSU. Various randomized, placebo-controlled studies reported that montelukast provided symptom alleviation in CSU patients when used as a monotherapy or in conjunction with cetirizine or desloratidine, but another placebo-controlled study demonstrated that montelukast plus desloratidine was equal to desloratidine alone while montelukast monotherapy offered no benefit over placebo [141, 144–146]. Another leukotriene receptor antagonist, zafiruklast failed to show benefit over placebo in CSU [147]. Some studies have only shown a benefit with leukotriene receptor antagonists in a subset of CSU patients with a positive ASST [148, 149]. Overall, leukotriene receptor antagonists may be added to anti-histamines in urticaria patients as a limited trial and have a side effect profile similar to placebo.
Systemic corticosteroids also have a role in severe, antihistamine-resistant CSU when rapid control is warranted or with episodes of significant angioedema. The mechanism for disease alleviation with corticosteroids is not known, but CSU patients treated with steroids have a transient rise in peripheral basophil counts perhaps suggesting decreased recruitment of basophils to the skin [70]. The use of systemic corticosteroids should be sparse due to the side effect profile with prolonged use including a greater risk for osteoporosis, peptic ulcer disease, diabetes, and hypertension, to name a few [150].
More recently, anti-inflammatory drugs have been used for the treatment of antihistamine-unresponsive and steroid-dependent CSU. In various case reports, sulfasalazine has shown some benefits in CSU as well as delayed pressure urticaria [151–154]. One recent study of patients with antihistamine-unresponsive CSU reported that 74 % of patients treated with sulfasalazine had significant improvement in disease and with an additional 21 % showing minimal improvement, and in additional all patients treated either discontinued or decreased their steroid use [155]. Although the mechanism of action is unknown, it is hypothesized that sulfasalazine may alter IgE-mediated mast cell histamine release, with one study demonstrating reduced release in mast cells and two prior studies demonstrating enhanced release in mast cells as well as basophils [156–158]. Dapsone, which exhibits anti-inflammatory properties and inhibits neutrophil function, showed promising results in one open-label study and may be beneficial for patients with neutrophil-predominant infiltrates on skin biopsy [159, 160]. More recently, a small randomized placebo controlled trial showed benefit in patients with antihistamine-refractory CSU [161]. This medication should be avoided in individuals with G6PD deficiency, which places patients at risk for hemolytic anemia [150].
Hydroxychloroquine has also shown some benefit in chronic urticaria. A randomized, double-blind, placebo-controlled study showed a significant improvement in quality-of-life scores in patients treated with hydroxychloroquine, but only a marginal change in urticaria activity scores [162]. Hydroxychloroquine has a number of immunologic effects, which include inhibition of endosomal TLR signaling resulting in reduced B-cell and dendritic-cell activation, as well as inhibition of antigen presentation [163]. In vitro studies have shown that hydroxychloroquine can decrease the production of TNF-α, IL-6, and IFN-γ by mitogen-stimulated peripheral blood lymphocytes [163, 164]. When compared with other immunomodulatory agents, antimalarials have a favorable safety profile [163]. Although rare, there is a risk of retinopathy with prolonged use (>5 years) of hydroxychloroquine [150].
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


