Chapter 28. Alar Base Modification
 Indications: The alar base includes the alar rims as they begin medially at the tip and columella and curve laterally to end at the attachments to the cheek. Ideally, the alar base of the nose should approximate an equilateral triangle with a slight degree of convexity at the alar cheek junction (Figure 28-1). It should provide adequate support to prevent collapse of the external nasal valve and demonstrate minimal scarring. Each has a cutaneous outer portion and an inner vestibular portion with a greater or lesser amount of intervening soft tissue. Preoperatively, the frontal view should identify the width of the alar base (Figure 28-2). Each side should be carefully examined in tandem, as well as separate from one another. In general, the alar bases are slightly wider than the distance between the medial and lateral canthi and should not extend past a vertical line dropped from the medial canthus. Excessive flaring or convexity of the alar bases should be documented if present. The lateral view will identify the cranial-caudal position of the alar base. It will also highlight the position of the alar rim and the columella separately and as they relate to one another (this will be examined separately in the following section). Finally, the basal view will identify the size of the nostril openings and the degree of flaring on each side. The long axis of the nostril should be at a 50- degree to 60-degree angle off a vertical line through the columella, and the nostril to tip proportion should be about 60:40 to 55:45. With careful inspection and palpation, the examiner should judge the quality of the skin and underlying soft tissue. The outer cutaneous surface should be considered separate from the inner vestibular surface. Any external or internal scarring of the skin and/or mucosa should be noted. In some patients, the nostril size and shape are adequate, but the overall inter-alar width is excessive on account of an excessively thick alar rim. In these patients, resection of a greater width of the cutaneous surface versus the vestibular surface might be indicated. Antero-posterior, oblique, lateral, and most importantly, worm’s eye views on preoperative photographs are critical to highlight the characteristics of the alar complex.
Indications: The alar base includes the alar rims as they begin medially at the tip and columella and curve laterally to end at the attachments to the cheek. Ideally, the alar base of the nose should approximate an equilateral triangle with a slight degree of convexity at the alar cheek junction (Figure 28-1). It should provide adequate support to prevent collapse of the external nasal valve and demonstrate minimal scarring. Each has a cutaneous outer portion and an inner vestibular portion with a greater or lesser amount of intervening soft tissue. Preoperatively, the frontal view should identify the width of the alar base (Figure 28-2). Each side should be carefully examined in tandem, as well as separate from one another. In general, the alar bases are slightly wider than the distance between the medial and lateral canthi and should not extend past a vertical line dropped from the medial canthus. Excessive flaring or convexity of the alar bases should be documented if present. The lateral view will identify the cranial-caudal position of the alar base. It will also highlight the position of the alar rim and the columella separately and as they relate to one another (this will be examined separately in the following section). Finally, the basal view will identify the size of the nostril openings and the degree of flaring on each side. The long axis of the nostril should be at a 50- degree to 60-degree angle off a vertical line through the columella, and the nostril to tip proportion should be about 60:40 to 55:45. With careful inspection and palpation, the examiner should judge the quality of the skin and underlying soft tissue. The outer cutaneous surface should be considered separate from the inner vestibular surface. Any external or internal scarring of the skin and/or mucosa should be noted. In some patients, the nostril size and shape are adequate, but the overall inter-alar width is excessive on account of an excessively thick alar rim. In these patients, resection of a greater width of the cutaneous surface versus the vestibular surface might be indicated. Antero-posterior, oblique, lateral, and most importantly, worm’s eye views on preoperative photographs are critical to highlight the characteristics of the alar complex.
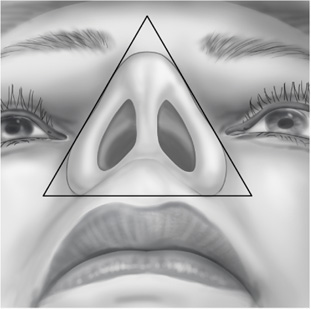
Figure 28-1. Worm’s eye view demonstrating the roughly equilateral triangle of the alar base.
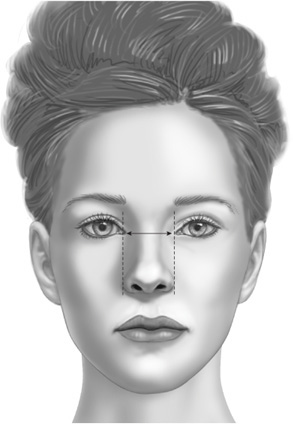
Figure 28-2. The alar width should approximate the distance between the medial canthi.
 Markings: The preoperative markings are important to ensure the appropriate amount of tissue is resected. In patients with more malleable skin and soft tissue, the alar base can be gently grasped and advanced towards the cheek to give the surgeon a rough idea of the amount of resection that is both needed and tolerable without undue tension. Calipers should be used to carefully measure the amount of tissue to be excised (Figure 28-3). Certainly, in instances where there is an unequal nostril size, differing amounts of tissue can be resected. Two curvilinear lines are marked on the cutaneous surface perpendicular to the alar rim. The lines will converge over the surface of the nose before advancing onto the nasal sidewall. They should not extend superior to the alar crease to avoid injury to the lateral nasal vessels.1 The incision should be made 1 mm above the alar-cheek junction to preserve the curvature of the rim and avoid having the scar fall within the alar crease. Variable amounts of lining skin and mucosa can be removed.
Markings: The preoperative markings are important to ensure the appropriate amount of tissue is resected. In patients with more malleable skin and soft tissue, the alar base can be gently grasped and advanced towards the cheek to give the surgeon a rough idea of the amount of resection that is both needed and tolerable without undue tension. Calipers should be used to carefully measure the amount of tissue to be excised (Figure 28-3). Certainly, in instances where there is an unequal nostril size, differing amounts of tissue can be resected. Two curvilinear lines are marked on the cutaneous surface perpendicular to the alar rim. The lines will converge over the surface of the nose before advancing onto the nasal sidewall. They should not extend superior to the alar crease to avoid injury to the lateral nasal vessels.1 The incision should be made 1 mm above the alar-cheek junction to preserve the curvature of the rim and avoid having the scar fall within the alar crease. Variable amounts of lining skin and mucosa can be removed.
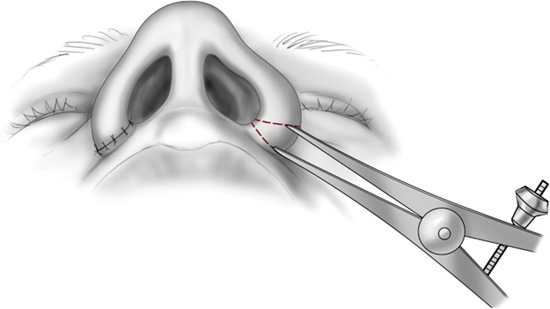
Figure 28-3. Measuring the contralateral alar rim so that symmetrical amounts of skin and soft tissue are removed.
 Technique: Several alar rim deformities can been encountered. Their characteristics and treatment are discussed below.
Technique: Several alar rim deformities can been encountered. Their characteristics and treatment are discussed below.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


