(1)
University of Pittsburgh Medical Center, Pittsburgh, PA, USA
2.1 Aesthetic Surgical Anatomy
The objective of body-contouring surgery goes beyond removal of loose skin and lifting ptotic structures. The goal is aesthetic topographical anatomy that is pleasing to the patient. Aesthetic surgical anatomy is a noticeable feature that a surgeon has the skill to modify or create. In a properly selected and prepared patient, the optimal result is achieved through an idealized vision executed by appropriate technique and postoperative care. Thoughtful excisions are designed. Precise incisions are expeditious and atraumatic. Flaps are mobilized with preservation of neurovascular. Contiguous liposuction preserves the subcutaneous architecture. Autogenous tissue augmentation is often better suited than implants. With an immense experience in body-contouring surgery over the past decade, new procedures have been adopted, modified, or innovated with improved skills to produce desirable aesthetic anatomy.
An appreciation of idealized gender-specific, surgical aesthetic anatomy is useful. Throughout a patient evaluation, the surgeon is mindful of these aesthetic ideals that must be resolved to musculoskeletal realities, tissue elasticity, and patient expectations. Otherwise, as my revered University of Pittsburgh plastic surgeon chief Willie White taught, “If you aim at nothing, you will hit it every time.”
There are well-recognized musculoskeletal, skin adherence, and fat distribution gender differences. These distinctions should be discriminating goals. Since massive weight loss and aging tend to masculinize women and feminize men, a major objective is to reverse gender dysmorphia. Nevertheless, there are many limitations to achieving aesthetic outcomes. Foremost are fear of surgery and patient financial constraints. The patient’s underlying musculoskeletal frame can be an issue. Broad ribs, a narrow pelvis, or a high arching pelvic rim forms a short waist, which cannot be fully overcome by reducing superficial soft tissues. Endomorphs, mesomorphs, and ectomorphs each have limitations and special opportunities for body shaping. Seemingly extraneous issues such as subclinical malnutrition, chronic disease, aversion to scars, and avoidance of risk or pain can significantly constrain outcomes. Interplay of neighboring aesthetic regions is always a difficult challenge. Patient refusal of revision surgery may leave iatrogenic deformity.
A request for body contour surgery prompts a thorough aesthetic, medical, and motivational assessment. That assessment matches deformity with patient goals. Patients usually notice contour and skin laxity of the anterior torso, thighs, and arms. Not so readily visible are other areas like the back, lateral breasts, and buttocks. These areas may not be a major concern, or the patient simply does not appreciate there are treatments. A complete approach to the body-contouring patient is similar to the dealing with facial rejuvenation. It is expected that the surgeon present a global view by including the eyelids, brows, and lips in addition to tightening the sagging neck and jowls. The patient is alerted that correcting one area of anatomy may make untreated areas more obvious and place facial features out of harmony. For the past 10 years, all of patients requesting body contouring receive a copy of Total Body Lift (Hurwitz 2005). That book provides the total scope of the issues through the experience of a plastic surgeon and the testimonials of treated patients. Recently, the American Society of Aesthetic Plastic Surgery Smart Beauty Guide (2013) for prospective patients borrows the term total body lift (TBL) to describe comprehensive body contouring after massive weight loss. That term was introduced by this author (Hurwitz 2004) and has continued to be used in all related publications and presentations over the past decade. TBL concept has gone main stream.
When TBL surgery is fully presented, the patient will understand optimal treatment. The patient can then accept most or the entire plan. An initial limited approach is sometimes expanded years later when the patient returns for further surgery. While advantageous for all patients seeking body contouring, the comprehensive approach is essential after massive weight loss (MWL).
2.2 Relevant Female Aesthetics
As Western society fashionably exposes or tightly clothe much of women’s surface anatomy, women understandably consider body contour surgery more often than men do. Beautifully shaped and proportioned women appear in a variety of presentations. We know when we see one. When beauty is lacking, the plastic surgeon must understand the variance; imagine the impact of surgery on creating features that are more desirable and then execute the complex changes in an efficient manner.
Women have a relatively small musculoskeletal frame that is broadest across the lower torso and upper thighs (Fig. 2.1). Most desirable is the hourglass figure with a smooth thin abdomen and waist that expands inferiorly to a broad pelvis and progressively tapers superiorly up the chest to rounded shoulders not quite as wide at the hips. Ideally, a slightly convex back leads to a deep lumbar lordosis that straightaway expands to buttock convexity. The highlights are well-defined high-positioned breasts and broad buttocks.
Fig. 2.1
Frontal, left anterior, and posterior oblique drawings of a 38-year-old mother with ideal body contours after comprehensive body-contouring surgery
A reasonable candidate for this transformation is a 39-year-old, 5’ 4”, 142 lb mother who sought a breast lift and abdominoplasty after losing 30 lb through dieting and exercising (Fig. 2.2). She was marked for a Wise pattern mastopexy with Quill suture suspension and lipoabdominoplasty including ultrasonic-assisted lipoplasty (UAL) of the hips and flanks. A #2 PDO barbed suture suspension of the central posterior breast to the pectoralis muscle was seen 1 week later to correct her nipple ptosis, overfill her superior and empty her inferior breast poles, and raise her breast footprints and inframammary folds (Fig. 2.3). With settling, the inferior poles of the breasts filled out and the shapeless torso was sensuously shaped as photographed 24 months later (Fig. 2.4). Given her excellent underlying musculoskeleton, and a thorough sculpting of her lower torso adiposity, anterior skin excess, and reshaping of her breasts, an exceptionally attractive outcome was achieved.

Fig. 2.2
Frontal, left anterior, and posterior oblique views of the 38-year-old mother in Fig. 2.1 with presurgical markings of Wise pattern mastopexy, abdominoplasty, and UAL of the trunk. The mastopexy was supported with #2 Quill from the second through 6th ribs, which is marked on the patient’s chest. 600 cc of fat was removed by UAL from each flank and 400 cc from the epigastrium
Fig. 2.3
Left anterior oblique view 1 week after comprehensive single-stage surgery designed and described in Fig. 2.2. The breasts are temporarily overfilled in the upper poles and underfilled in the lower poles. There is temporary gathering of the superior flap of the abdominoplasty. The umbilicus and flanks are swollen
Her defining femininity is maximum fullness across the buttocks and hips framed by spinal, flank concavity and flat posterior and lateral thigh contours. Prominently symmetrical rounded but slopping breasts surrounded by well-defined inframammary folds (IMF) balance her lower torso curves over the sternum and lateral chest (Fig. 2.4). The depth of midlateral torso, between the iliac crests and costal margins, i.e., the waist, depends on skeletal relationships and accumulation of skin and fat. A narrow-based neck leads to small angular shoulders that continue to upper arms tightly enwrapping subtle muscular curvature. The broad muscles of the female back are too thin to obscure scapular edges or deep curves of the lumbothoracic spine.
Women’s upper arms are tapering undulating cones extending from shoulders to elbows. A recent 1-year postoperative L-brachioplasty result in a thin and muscular 67-year-old woman demonstrates the salient aesthetics that applies across genders (Fig. 2.4). Her frontal and posterior images are all taken in standardized positions of the upper arm abducted 90° from the body and flexed at right angles with the arm supine. These are also the positions that the patient is asked to take when assessing redundancy of skin and fat. The elbow is not extended, because the skin laxity about the elbow slides to the distal arm. Her preoperative views demonstrate mild hanging skin laxity, unacceptable to the patient (Fig. 2.5).
Fig. 2.5
Frontal and posterior views of ideal arm aesthetics, in a muscular 63-year-old woman. One year prior she underwent L-brachioplasty, leaving faint curvilinear medial scars
The arm is shaped by muscular and adipose disposition and mass (Fig. 2.5). There are two layers of fat. The subdermal areolar layer of vertically segmented adipose containing the superficial neurovasculature surrounds the arm. There is a lamellar layer (deep) composed of horizontally oriented adipose only posteriorly. This deep layer stores excess fat. Except for the thinnest women, muscular definition is muted by minimal muscular bulk and more fat in the areolar layer. Regardless, the ideal aesthetic result in either gender is tight skin enveloping muscular curves. The deltoid and biceps muscles clearly define the bulging curves of the anterior and external arms. Separated from the biceps and brachioradialis by transverse grooves, the hanging triceps supplemented by a deposit of lamellar fat imparts a central convexity to the posterior arm. This muscle, with tightly adherent skin, acutely rises to attach to the chest to create the posterior axillary fold. The width of the most proximal arm from its attachment to the chest and the deltoid prominence is equal to the midarm from the deepest curvature of the triceps to the bulge of the biceps. The relatively flat internal arm is accentuated by the bicipital groove which leads to the axilla.
The axilla is a shallow dome created by the suspended clavipectoral fascia and bordered by the triceps, latissimus dorsi, and pectoralis muscles. There is a dynamic aesthetic relationship of the depth of the axilla to the position of the arm. As the arm rises from resting against the chest to full abduction and extension, the axillary recession increases to its greatest depth at 90° of abduction and progressively flattens as the arm is further raised. The clavipectoral fascia roof recesses the central axilla. The adherent hair-bearing skin is tethered by fascia extensions through the lymph nodal area to the upper chest. Massive weight loss dramatically increases axillary depth and size. Despite excellent muscular development, aging leaves lax skin throughout the arm (Fig. 2.6). That undesirable laxity from elbow through lateral chest was treated with an L-brachioplasty, leaving only a fine line curvilinear medial arm scar that crossed the axilla onto her lateral chest (Fig. 2.5).
Fig. 2.6
Frontal and posterior views of a 63-yearold muscular woman requesting reduction of sagging arm skin 1 year prior to the result seen in Fig. 2.5
The upper torso consists of upper back, rib cage, and breasts. Spinal curvature with paraspinous muscular ridges and the scapulas are defining features, while the great superficial flat trapezius, latissimus dorsi, and pectoralis muscles are barely perceptible (Fig. 2.1). The lateral breasts smoothly taper along and obscure the anterior axillary fold created by the edge of the pectoralis major muscle. Springy breasts emerge between this lateral border and the sternum. The soft breast mounds arise from proportionate nipple areolar complexes (NACs) capped by the small central projecting nipples, at the most forward point. Streaming fascia strands (Cooper’s ligaments) provide loose attachment to anterior chest muscles. There are many forms of attractive breasts, but most slope from superior to a fuller lower pole. The rounded lower pole abruptly ends at the IMF. The medial and lateral margins are nearly as well defined.
Continuing through the lumbar region, the central back becomes deeply concave with two accompanying ridges that end together as a dramatic rise to the sacrum. The rounded hips flare at both sides. Each buttock rises to a round central convexity. The superior or inferior perimeters may taper inward. The inferior medial buttock abruptly ends at the posterior thigh, while the lateral buttock smoothly tapers to the posterior thigh. The posterior thigh is flat with the lateral aspect tapering from the trochanter prominence to the knee.
Directly anterior to the buttock prominence is the center of the mons pubis. Its gentle convexity continues from the slightly round lower abdomen. The mons pubis tapers laterally to the flat groins and inferiorly to the rounded prominences of the labia majora. There is distinct upper thigh-labia majora junction. The anterior thigh can be slightly full and taper to the knee. Finally, the upper abdomen is flat from xyphoid to umbilicus. The midline linea alba, the transverse inscriptions, and lateral rectus muscle depressions are subtle.
Unless exceptionally lean and athletic, women have subtle definition of the muscles of the trunk for two reasons. Without high levels of circulating testosterone, muscular bulk is difficult to develop. Moreover, women have even and thick layers of adipose deep to both Scarpa’s and muscular fascias. Women have focal increased fat deposition of the breasts, lower abdomen, hips, buttocks, and thighs. This pattern of fat deposition leads to contours and suppleness related to localized fat stores not muscularity. With weight gain and after menopause, women tend to layer adipose disproportionately in these subcutaneous layers as well as lateral to the breasts, mid back, flanks, and upper arms.
2.3 Relevant Male Aesthetics
Men are more broad across rounded shoulders and upper body (Fig. 2.7). Relatively narrow hips lead to rounded firm buttocks and tapering muscular thighs. Ideal male shape is dominated by the upper body musculoskeletal development with definition reflected through tight skin and highlighted by strategic adherences. The defining upper body masculine features are the broad and flat superficial trapezius, latissimus dorsi, and pectoralis major muscles. The trapezius fans out from the base of the skull to broaden the neck base to the shoulders. Along with the latissimus, these muscles flatten and broaden the back, obscuring borders of the scapula and softening the spinal curvature. Inferior to the lateral costal margins, the waist subtly narrows to gently expand for the pelvic rims.

Fig. 2.7
Left anterior oblique torso view post total body lift surgery in a muscular male. Optimal pectoralis muscle to chest wall skin relationships is seen in this 41-year-old massive weight loss patient with raised arms 4 years after boomerang pattern correction of gynecomastia, upper body lift, and posterior extended abdominoplasty. The aesthetic rolls and adherences are labelled. The new nipple positions are just superior to the inferior border of the pectoralis muscles. Long but faint surgical scars hang over the nipple areolar complexes (NAC) to descend obliquely to the 8th costochondral junction and ninth rib along the midlateral chest
In contrast to the sloping and rounded female breast obscuring pectoralis major, that muscle dominates the ideal male anterior chest (Fig. 2.7). The pectoralis major originates from lower ribs and spans the upper anterior thoracic cage to insert on the clavicle and superior humerus. Upon extension of the arm, the stretched pectoralis muscle leaves no fullness inferior to the nipple. The developed pectoralis muscle is a flat superficial muscle imparting an unevenly projecting rhomboid that impressively changes contour with contraction. At rest, it smoothly fills behind the nipple (Fig. 2.8, upper). The contracting pectoralis bulges the midportion of the chest while inferior to the nipple empties (Fig. 2.8, lower). The obliquely aligned thick lateral pectoral border dominates the span at rest and more so when the arm is abducted. The lateral border is accentuated by the triangular depression over the thin serratus anterior muscle leading to the raised lateral border of the latissimus dorsi muscle. The superior parasternal and infraclavicular regions are slightly depressed. Tightly adherent skin reflects pectoral muscular bulk with depressed demarcation along the lateral border and inferior attachment to the chest. There is no inframammary fold because the mammary gland is not developed. As such, once the gynecomastia is corrected, plastic surgeons should not be trying to create an IMF. Nor should there be any infra-areolar bulk as created by a deepithelialized inferior pedicle to the NAC (Gusenoff et al. 2008).
Fig. 2.8
Frontal views standing 4 years after Fig. 2.9 showing well-developed pectoralis muscles relaxed (above) and contracted (below). At rest, the pectoralis muscles fall into the infra-areolar skin envelop, stopped by a well-defined skin adherence along the infra-lateral muscle. The fully contracted pectoralis muscles bulge skin superior to and empty skin inferior to the slightly rising NACs. Residual gynecomastia, generalized loose chest skin, or a buried skin flap would obscure this effect
Descending from the chest is the central 6 pack of the rectus muscle. Aside for the small bulge of the external oblique, the waist is narrower than the pelvic rim. The converging latissimus emphasizes the dominance of the upper body. Slightly rounded firm buttocks lead to conical muscular thighs.
Five years before the taking of images (Figs. 2.7 and 2.8), the ideal male underwent a total body lift consisting of boomerang pattern correction with back extensions and an abdominoplasty with flank extensions (Fig. 2.9). This body builder exemplifies that complex attractive male anterior chest aesthetics can be surgically restored. After a 75 lb weight loss, this 5’ 10”, 185 lb part-time warehouse fighter was embarrassed by sagging gynecomastia. He was discouraged that his upper body building failed to show pectoralis muscle enlargement. He has sagging breasts overlapped well-defined inframammary folds. Loose anterior chest skin obscures pectoralis muscle features. He has loose skin and excess fat of the lower abdomen and flanks. To avoid having his loose chest skin grabbed during a match, he needed the skin wrapped tight. The boomerang pattern combines correction of gynecomastia with an upper body lift (UBL) and elevation of his nipples on an inferior skin pedicle to the lower portion of the pectoralis muscle. The oblique ellipses joined at right angles over the nipple to remove all excess chest skin vertically and horizontally. The result 4 years later shows correction of his gynecomastia and taut skin across the chest to reveal details of resting and contracted pectoralis muscles (Figs. 2.7 and 2.8). The chest scars are no more visible than his residual stria. His defined low-lying IMFs have been eliminated by superior anchoring of the UBL and discontinuous undermining throughout the abdominoplasty. Technical details are presented in Chap. 5.
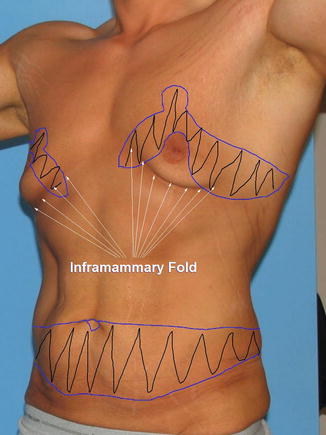
Fig. 2.9
Left anterior oblique view of preoperative torso of patient shown in Figs. 2.7 and 2.8. The gynecomastia is thin, flat, and ptotic with inframammary folds noted below the inferior border of the pectoralis muscle. A boomerang pattern correction with a left back extension and an abdominoplasty with flank extension are drawn on the image. The new nipple position is sited superior to the inferior attachment of the pectoralis muscle and medial to the lateral roll
2.4 Evaluating Disordered Female Anatomy
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


