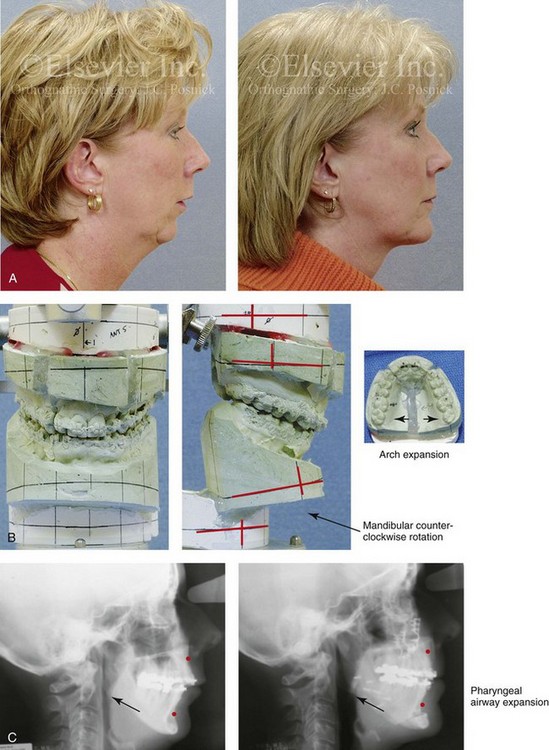
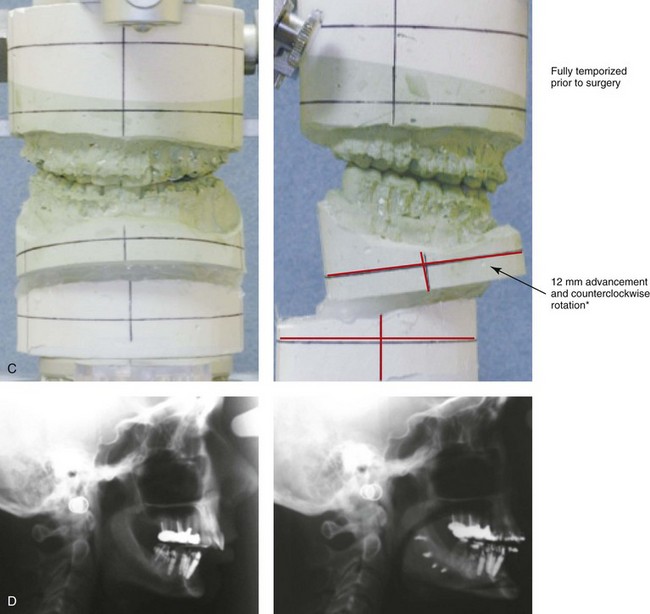
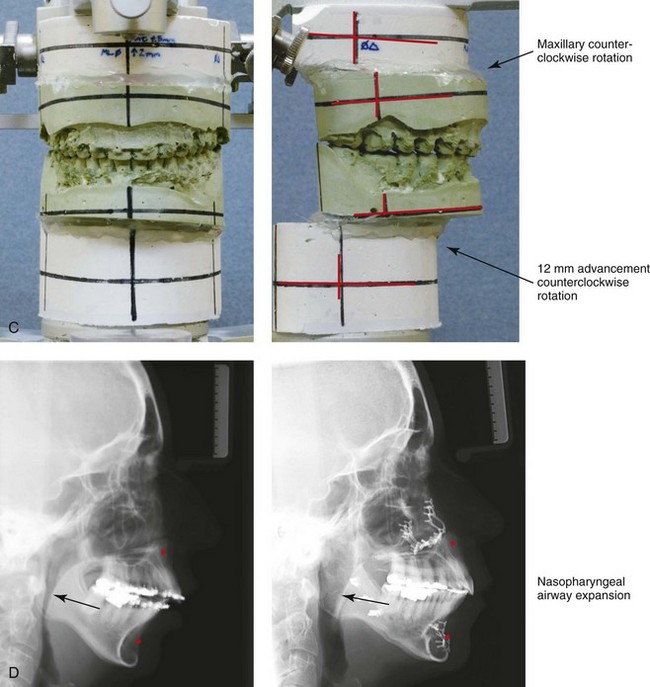
40 I agree with Fritz Barton when he stated the following: “The shape of the human face is composed of a skeletal bony framework that is covered by a soft tissue envelope. Overall, skeletal proportions are probably the most important component of facial attractiveness.”7 In my experience, the absence of an attractive cervical–mental (neck–mandibular) angle most often is the result of a developmental mandibular deficiency that predisposes the affected individual to loose lower cheek and neck skin, the noticeable bunching of fat in the neck area, and the eventual presence of visible platysma bands that worsens and becomes less attractive with age (see Chapters 19, 23, and 25). The layers of the face encompass the skin; the underlying soft tissues, including the fat (subcutaneous and deep); the mimetic muscles (superficial and deep); the investing fascia, which is known as the superficial muscular aponeurotic system (SMAS); the retaining ligaments; and the skeletal structural support system (bones, cartilage, and teeth).4,18 The soft tissues of the face will naturally descend with age, which will result in progressive laxity and ptosis of the skin, the subcutaneous tissue, the fat, and the fascia (i.e., the SMAS–platysma layer) as well as the retaining ligaments. The facial fat (subcutaneous and deep) may either atrophy (i.e., as a result of resorption) or hypertrophy (i.e., increase in volume), and it is also affected by gravity over time. Facial aging is dynamic and cumulative, and it is also affected by hormonal and degenerative changes in the soft tissues. An understanding of the pertinent biochemical and histologic changes that tend to occur in the facial soft tissues with age and through environmental exposures is an important aspect to consider when developing a reconstruction and rejuvenation treatment plan. Soft-tissue aging is affected by genetic aspects, hormonal changes, and environmental influences. For some individuals, the deeper soft-tissue envelope remains well preserved while the superficial surface of the skin appears weathered. For others, the surface skin remains youthful while the deeper soft-tissue envelope loses structural landmarks with cutaneous laxity. Extrinsic (environmental) forces that are working on the skin include dehydration, inadequate nutrition, temperature extremes, traumatic influences, chronic exposure to strong ultraviolet sunlight, toxins (e.g., cigarette smoke), and gravity. The intrinsic (genetic) effects have to do with the individual’s basic soft tissues and their skeletal morphology.15,73 Environmental (extrinsic) factors primarily result in dysplasia and structural alteration of the dermal and epidermal layers of the skin, whereas intrinsic (genetic) effects on the skin may result in atrophy and the loss of structural dermal and epidermal components.19,20,29,84 An individual’s hormone levels throughout life are also known to have significant effects on the aging process.30 Aging is associated with declining levels of several hormones, and it is gender dependent. It is known that, in women, declining estrogen levels are associated with cutaneous changes, many of which can be reversed or improved via estrogen supplementation. Studies of postmenopausal women indicate that estrogen deprivation is associated with dryness, atrophy, fine wrinkling, poor healing, and hot flashes.30,60 Epidermal thinning, declining dermal collagen content, diminished skin moisture, tissue laxity, and impaired wound healing have been reported among postmenopausal women. The soft-tissue effects of changing hormonal levels with age in males are less well studied but presumed to be of equal importance. The cumulative intrinsic (genetic) effects on the skin can be seen histologically as epidermal thinning, changes in the morphology of the keratinocytes, and a decrease in the number of Langerhans cells and melanocytes. Environmental (extrinsic) aging effects on the skin result in keratinocytic dysplasia and the accumulation of solar elastosis, and they can result in cutaneous carcinogenesis (e.g., basal cell carcinoma, melanoma, squamous cell carcinoma). All individuals experience some degree of both extrinsic (environmental) and intrinsic (genetic) aging simultaneously (Fig. 40-1). The genetic variability of an individual’s skeletal framework and the degree and pace of soft-tissue aging in each tissue layer makes a uniform template for facial rejuvenation impractical. Visually, as the intrinsic and extrinsic aging of the skin progress, there will be pigmentary abnormalities, wrinkles (rhytids), and texture irregularities that may result in a “weathered” appearance. Current thinking about aging also involves the concept that the gain or loss of fat volume within the deep compartments leads to changes in the shape and contour of the face.20 By contrast, soft-tissue folds occur at the transition points between the thicker and thinner superficial fat compartments. The transition points cause nasolabial folds, labiomental folds, submental creases, and preauricular folds.65,67 In the upper third of the face, around the eyes, researchers have found that suborbicularis oculi fat is composed of two distinct anatomic compartments: the medial limbus and the lateral canthus region. These researchers have also confirmed that the lateral suborbicularis oculi fat extends from the lateral canthus to the lateral orbital thickening.7 The deep medial cheek fat is the most medial of the periorbital deep fat compartments.51 In current clinical practice, periorbital rejuvenation relies more on soft-tissue augmentation and rearrangement than on tissue removal. In the midface, progressive skin laxity is often combined with the resorption of subcutaneous fat and gravitational effects to result in characteristic changes in the soft-tissue envelope.65 In the lower third of the face, there may be ptosis of the chin soft tissues, a loss of the delineation between the jawline and the neck, the development of characteristic jowls, and looseness in the neck skin (which, in the extreme, is characterized as resembling a “turkey gobble”). In many individuals, prominent vertical platysma bands develop in the submental region, and there is often fat hypertrophy in the submental and submandibular regions. These aging effects further hide or eliminate an otherwise attractive and youthful neck–jaw angle. Figure 40-1 A 46-year-old woman first arrived for the surgical assessment of a longstanding bony mass in the left forehead region. She underwent a computed tomography scan that confirmed an osteoma without intracranial involvement. She elected to not undergo biopsy, recontouring, or removal at that time. She returned 13 years later, when she was 59 years old, to discuss facial aging. Her concerns included webbing (platysma bands) and loose skin of the neck; heavy jowls; marionette lines; deep nasolabial folds; puffiness and irregularities of the lower eyelids; hollowing in the temporal and cheek regions; deepening of the labiomental crease; and vertical wrinkles of the upper lip. She had undergone Restylane injections of the nasolabial folds, the marionette lines, the labiomental crease, and the lower eyelids with another clinician but without satisfactory improvement. She also had a short face growth pattern (i.e., maxillomandibular deficiency). During her teenage years, she had undergone camouflage orthodontic treatment that included upper bicuspid extractions to achieve a neutralized occlusion. There was no dental show with the upper lip in repose. With broad smile, only half of the maxillary incisors were visible. The upper lip appeared to have lengthened slightly, and the lips appeared to be more deflated (as compared with images taken when the patient was 46 years old). She stated that she received frequent comments about looking “sad” or “unhappy.” She had a history of an inability to breathe well through the nose, loud snoring, restless sleeping, and excessive daytime fatigue. An attended polysomnogram was carried out and confirmed obstructive sleep apnea, with a respiratory disturbance index of 24 events/hour with desaturations of up to 85%. A comprehensive approach to improve dental health, open the upper airway, and enhance facial aesthetics was planned (see Chapters 23 and 25). A, Frontal facial views at 46 and 59 years of age. B, Oblique facial views at 46 and 59 years of age. C, Profile facial views at 46 and 59 years of age. • Forehead (horizontal) and glabellar (vertical) creases • Ptosis (drooping) of the lateral eyebrows • Lower eyelid laxity and wrinkles • Lower eyelid (puffy) visible bags • Deepening of the nasojugal grooves and the palpebral malar grooves • Ptosis (drooping) of the malar soft tissues • Generalized facial skin laxity* • Deepening of the nasolabial folds* • Loss of neck definition (neck–jaw angle) and excess fat collection (hypertrophy) in the neck* • Deep platysmal bands that are visible in repose and often more obvious with function (e.g., facial expression)* • Downturn of the oral commissures The goal is to help the individual look more like the way they used to look rather than severe, operated on, or unnatural.44,79,94,95 The recognition of any longstanding maxillomandibular skeletal disharmonies is essential to the achievement of enhanced facial aesthetics. If the surgeon attempts to ignore baseline skeletal deformities and then overcompensates with excessive soft-tissue maneuvers, the outcome is likely to be suboptimal. Amateurish or overdone face lifts often look excessively taut, radically defatted, or overfilled (e.g., fat grafts, artificial fillers), or they may involve irregularities from deep layer soft-tissue manipulation. The “overoperated” face may also look startling and unnatural from too much soft-tissue surgical alteration in just one region or layer of the face while ignoring the others. The entire face and all of its layers should be analyzed and given consideration before focusing on just one aspect or technique for rejuvenation. Throughout the body, the soft tissues external to the skeleton are anchored to the bony framework by osseocutaneous ligaments that pass directly from the dermis to the periosteum in bare areas where there are no muscles that separate them.22,39,49,62,63,67,80 The most prominent of these retaining ligaments in the head and neck are in the cheek and along the lateral border of the mandible. The retaining ligaments that partition the cheek fat from the neck are called the mandibular septum. A face lift that simply undermines the cheek soft tissues followed by excessive skin resection and then wound closure under tension does not simultaneously manage the deeper soft tissues. Therefore, in these circumstances, skin undermining and resection alone will rarely achieve an attractive or youthful face. This limited “skin-only” approach to face lifting with excessive skin resection may also lead to unsightly scars, flap necrosis, or, more commonly, distortions of key landmarks with the loss of the natural facial curvatures. The use of face-lift techniques that also modestly redistribute the deep soft-tissue layers (i.e., the SMAS–platysma layer) in combination with conservative skin removal and relaxed wound closure will often result in the more pleasing contours that are associated with a youthful and attractive appearance. The process of aging involves not only gravitational effects on the soft tissues and degenerative changes of the skin but, in many cases, noticeable soft-tissue volume loss (deflation) through the atrophy (resorption) of the fat.10,29,42,66,68,70,72,81 Frequent visual effects of descent in the face include the deepening of the nasolabial folds, ptosis of the malar portion of the superficial fat, and the accumulation of fat in the jowls. The classic effects of deflation are seen most frequently in individuals who have had lifelong thinness of the face. The fat atrophy in these individuals is often visually seen in the temporal fossa, periorbital, buccal, and perioral regions. In other individuals, a pattern of simultaneous face and neck fat hypertrophy as a result of weight gain will occur with age. To avoid an amateurish face lift, a good general rule for the surgeon to follow is to only cautiously remove any fat above the inferior border of the mandible and to be sure that an appropriate amount of fat is removed below the mandibular inferior border. Although adding fat to atrophied regions of the face is beneficial in principle, in many individuals, the long-term success of these techniques (i.e., autogenous fat grafting or the use of artificial fillers) to achieve a natural-appearing rejuvenation remains a work in progress.10 Face lifting will address gravitational changes in the soft-tissue envelope, but it does not have an effect on the quality of the soft tissues themselves.60,85 Face-lift procedures will not treat wrinkles (rhytids), sun damage, creases, or age-related pigmentation. If feasible, fine wrinkles and irregular pigmentation are treated with good-quality skin care and possibly resurfacing procedures (e.g., dermabrasion, chemical peel, laser). Preventative measures of avoiding excessive ultraviolet light exposure, cigarette smoke, temperature extremes, dehydration, and nutritional deficiencies are important. Significant variation occurs in the aging of each individual’s face and neck. Recognition that the shape of the neck is fundamentally determined by the maxillomandibular skeleton is essential (Figs. 40-1 through 40-4).13,16,24,32,69,71,93 The ideal neck configuration requires a well-proportioned facial skeleton; it is often described as having a cervical–mental (neck–jaw) angle of 105 to 120 degrees and a distinct mandibular inferior border. Interestingly, despite various assertions and opinions by a handful of authors, in the absence of a loss of the teeth or significant alteration of the dentition through either natural attrition or dental restorative procedures, no convincing data confirms significant changes in the maxillofacial skeleton with aging (see Chapter 25).* Figure 40-2 A woman in her mid 50s was referred from her general dentist to an orthodontist for the management of a longstanding Angle Class II excess overjet malocclusion that had gradually resulted in deterioration of the posterior dentition. The orthodontist recognized that the malocclusion resulted from a retrusive mandible and a constricted maxilla. With referral for surgical evaluation, the patient was found to have a developmental jaw deformity, chronic obstructed nasal breathing, and a sleep history that was consistent with obstructive sleep apnea. Unfavorable facial aging with a desire for an improved neck–chin angle was also discussed. An attended polysomnogram confirmed moderate obstructive sleep apnea. The patient agreed to proceed with orthodontic treatment that included lower first bicuspid extractions to relieve dental compensation in combination with jaw, intranasal, and facial surgery. The objectives were to open the upper airway, enhance the facial aesthetics, and achieve improved long-term dental health. The patient’s surgical procedures included maxillary Le Fort I osteotomy in segments (horizontal advancement, counterclockwise rotation, arch expansion, and correction of the curve of Spee); bilateral sagittal split ramus osteotomies (horizontal advancement and counterclockwise rotation); osseous genioplasty (horizontal advancement); anterior approach to the soft tissues of the neck (cervical flap elevation, neck defatting, and vertical platysma muscle plication); and septoplasty and inferior turbinate reduction (see Fig. 25-1). A, Profile views before and after reconstruction. Note the improved A-point–to–B-point relationship that was achieved as a result of maxillomandibular counterclockwise rotation. B, Articulated dental casts that indicate analytic model planning. C, Lateral cephalometric radiographs before and after surgery. Note the improved posterior airway space with pharyngeal expansion as a result of the orthognathic procedures. Figure 40-3 A woman in her early 50s was referred by a prosthodontist for surgical evaluation. There had been a gradual deterioration of the dentition, at least partially as a result of the longstanding skeletal Class II excess overjet deep-bite malocclusion. Head and neck evaluation confirmed a retrusive mandible that also resulted in retroglossal airway obstruction. A desire for improved profile aesthetics was also discussed. A comprehensive approach to dental rehabilitation, opening the upper airway, and facial rejuvenation and reconstruction was selected. Coordinated endodontic, orthodontic, periodontic, prosthodontic, and surgical care was required. Periodontal treatment, extractions, dental implant placement, restorative temporization, and orthodontic alignment were carried out. This was followed by surgery that included bilateral sagittal split ramus osteotomies (horizontal advancement and counterclockwise rotation); osseous genioplasty (vertical lengthening) with interpositional grafting; and an anterior approach to the soft tissues of the neck (cervical flap elevation, neck defatting, and vertical platysma muscle plication). This was then followed by crown lengthening and final dental restorations (see Fig. 25-6). A, Profile views before and after reconstruction and dental rehabilitation. B, Oblique facial views before and after reconstruction and dental rehabilitation. C, Articulated dental casts that indicate analytic model planning. D, Lateral cephalometric radiographs before and after reconstruction. Figure 40-4 A woman in her mid 50s was seen by a prosthodontist for the management of a deteriorating posterior dentition. She was confirmed to have secondary dental trauma as a result of a longstanding malocclusion. She was referred to an orthodontist and then for surgical assessment. Head and neck evaluation confirmed a short face growth pattern with a Class II excess overjet deep bite and constricted maxillary arch malocclusion. She had a lifelong history of obstructed nasal breathing, and her history was suggestive of obstructive sleep apnea (this was confirmed with an attended polysomnogram). Facial aesthetic concerns included downturned corners of the mouth, deep perioral creases, early jowl formation, weak profile, an obtuse neck–chin angle, and loose skin around the neck. The patient agreed to a comprehensive surgical and dental rehabilitative approach. Periodontal evaluation, initial restorations, and orthodontic decompensation preceded surgery. The patient’s surgical procedures included maxillary Le Fort I osteotomy (horizontal advancement, counterclockwise rotation, and vertical adjustment); bilateral sagittal split osteotomies of the mandible (horizontal advancement and counterclockwise rotation); osseous genioplasty (horizontal advancement); an anterior approach to the neck (cervical flap elevation, neck defatting, and vertical platysma muscle plication); and septoplasty, inferior turbinate reduction, and nasal recontouring (see Fig. 25-7). A, Oblique facial views before and after treatment. B, Profile views before and after treatment. C, Articulated dental casts that indicate model planning. D, Lateral cephalometric radiographs before and after treatment. Note the improved posterior airway space with pharyngeal expansion as a result of the orthognathic procedures. Face lifting was first performed during the early 1900s and involved skin incisions around the ears, limited skin-flap undermining, and then skin excision before wound closure. In 1859, Gray defined a unique deep layer of tissue just below the facial skin that was described as “superficial subcutaneous fascia.” Not much changed until the 1970s, when both Tessier and Skoog independently described the aesthetic benefit of manipulating this superficial subcutaneous fascia as a separate component during face lifting for rejuvenation purposes. The superficial subcutaneous fascia was recognized as investing the platysma muscles and fusing to the parotid fascia as the facial extension of the cervical investing fascia. It later came to be called the superficial muscular aponeurotic system or SMAS, as mentioned previously.48 The SMAS envelopes the platysma muscles within the neck and the lower cheek region. Superiorly, it terminates as the investing layer of the superficial mimetic muscles. Laterally, it fuses with the parotid capsule. Superiorly, it passes over the zygomatic arch to join the temporoparietal fascia. Tessier and Skoog were the first to include as part of the face-lift technique not just the undermining and excision of the skin but also the management of the so-called SMAS–platysma layer. This required unique incisions, undermining, redraping, and tightening of the SMAS–platysma as part of the face-lifting procedure. Since the initial contributions of Tessier and Skoog, every conceivable recommendation has been made by surgeons for dissecting, undermining, excising, adding to, or removing virtually all of the tissue layers and cell types in the head and neck to further enhance the aesthetic outcome.2–5,8,18,21,31,47,50,59,77,78 Many of the “innovations” in the area of face lifting have proven to have little additional long-term value, and some have resulted in increased complications and prolonged recoveries. This was confirmed by Chang and colleagues in a recently completed systematic review and comparison of efficacy and complication rates among a variety of face-lift techniques. The authors conclude that there are pros and cons to each of a variety of face-lift techniques and that there is no clear evidence that one is routinely superior to another.9 A well-designed traditional face lift often confers much benefit to the jowls (i.e., the mandibular line) and the neck (Figs. 40-5 through 40-10). It can be an effective way to soften the nasolabial folds, to lift the jowls back into the face, to relieve the platysmal bands, to remove the loose skin and excess fat of the neck, and to restore the neck–jaw angle back to its baseline. This can change the overall facial shape from rectangular back to that of a heart in a way that no other soft-tissue treatment modality can provide. The basic traditional face-lift approach requires the consideration of the following: Figure 40-5 A woman in her early 50s arrived for the evaluation of facial aging. She had satisfactory skeletal proportions and no significant surface skin layer aging effects. She requested surgery to diminish her jowls, to soften her nasolabial folds, and to reduce the amount of loose skin in her neck region. She underwent a face lift that included periauricular and submental incisions; cheek and neck flap elevation; superficial musculo-aponeurotic system flap elevation with postauricular transposition; neck defatting; vertical platysma muscle plication; and skin resection and redraping. Asymmetric upper eyelid ptosis was not addressed. A, Oblique facial views before and after surgery. B, Profile views before and after surgery. Figure 40-6 A 50-year-old woman arrived for the evaluation of facial aging. She has satisfactory skeletal proportions and minimal skin surface layer aging effects. She underwent a limited incision brow lift with suspension; blepharoplasty (elliptical excision of the upper eyelid skin and redraping of the lower lid tissue); and a face lift as described in the legend for Fig. 40-5. A, Oblique facial views before and after surgery. B, Profile views before and after surgery. Figure 40-7 A woman in her late 50s arrived for the evaluation of facial aging. She had satisfactory skeletal proportions but marked surface layer aging effects. She elected to not undergo skin resurfacing procedures. She agreed to a limited incision brow lift with suspension, blepharoplasty (elliptical excision of the upper lid skin and lower lid redraping), and a face lift as described in the legend for Fig. 40-5. A, Frontal views before and after surgery. B, Oblique facial views before and after surgery. C, Profile views before and after surgery. Figure 40-8 A woman in her early 40s requested an improved neck–chin angle and the relief of hooding of the upper eyelids. She had a short face growth pattern that resulted in mildly deficient lower anterior facial height and horizontal facial projection. She had a good airway and occlusion. There was limited surface skin layer damage and aging effects. She underwent upper blepharoplasty (elliptical skin incision) and a face lift as described in the legend for Fig. 40-5. A, Oblique facial views before and early after surgery. B, Profile views before and early after surgery. Figure 40-9 A woman in her early 50s with facial aging concerns. She had a mild long face growth pattern but a satisfactory occlusion. The lower anterior facial height was slightly increased, which resulted in mild lip incompetence and mentalis strain; this resulted in accentuated perioral creases. She agreed to blepharoplasty (elliptical excision of the upper lid skin and redraping of the lower lid tissue); osseous genioplasty (vertical reduction and horizontal advancement); and a face lift as described in the legend for Fig. 40-5. A, Frontal views before and after surgery. B, Profile views before and after surgery. Note the relief of the perioral folds and the mentalis strain as a result of vertical reduction and advancement genioplasty. Figure 40-10 A woman in her late 50s arrived for the evaluation of facial aging. She had satisfactory skeletal proportions and occlusion. Her skin was thick but did not have major ultraviolet light damage. She agreed to a limited incision brow lift with suspension; blepharoplasty (elliptical excision of the upper eyelid skin and fat removal and redraping from the lower lids); and a face lift as described in the legend for Fig. 40-5. A, Frontal views in repose before and after rejuvenation. B, Frontal views with smile before and after rejuvenation. C, Oblique facial views before and after rejuvenation. D, Profile views before and after rejuvenation. • Skin incision placement (i.e., preauricular with temporal extensions and postauricular with occipital extensions) • Skin flap elevation and undermining (i.e., temporal, cheek, postauricular, neck, and submental regions) • Supraplatysmal, intraplatysmal, and subplatysmal defatting (e.g., below the inferior border of the mandible and chin, above the thyroid cartilage, and anterior to and above the sternocleidomastoid muscles) • Platysma muscle management (i.e., vertical plication versus the excision of bands) • SMAS management (i.e., preauricular SMAS plication versus SMAS elevation with postauricular flap transposition) • Redraping of the elevated skin flaps (i.e., in a superoposterior vector) • Excision of redundant skin (e.g., temporal, preauricular, postauricular, occipital) Changes that occur in the neck with age can alter the natural youthful facial curvatures and angles.* As people age, characteristic changes tend to occur in the skin and throughout the soft-tissue envelope. Soft-tissue rejuvenation procedures that focus on the neck often include the following: 1) cervical flap elevation; 2) the selective removal of fat (above, in between, and below the platysma muscles); 3) the tightening of the platysma muscles (in the neck midline); and 4) the redraping of lax skin (i.e., skin retraction). In the presence of well-proportioned (harmonious) maxillomandibular skeletal structures, the combination of these procedures can generally be carried out to achieve a preferred geometric angle between the cylindrical neck and the straight-line inferior border of the jaw.12,18,23,25–27,34–36,41,46,61,83,94,95
Aesthetic Alteration of the Soft Tissues of the Neck and Lower Face
Evaluation and Surgery
Aging of the Facial Soft-Tissue Envelope
Background

Frequent Soft-Tissue Facial Aging Characteristics
Basic Principles of Midface and Neck Aging and Rejuvenation
Achieve Facial Harmony
Achieve Volume Redistribution rather than Skin Tension
Recognize the Presence of Fat Atrophy and Hypertrophy
Recognize Degenerative Changes in the Skin
Recognize the Negative Effects of Any Baseline Maxillomandibular Skeletal Disharmony


Approach to Rejuvenation Surgery of the Neck and Lower Face
Traditional Face-Lift Approach to Rejuvenation







Anterior Neck (Submental) Approach to Rejuvenation
Background
Related posts:
![]() Temporomandibular Disorders: Effects of Occlusion, Orthodontic Treatment, and Orthognathic Surgery
Temporomandibular Disorders: Effects of Occlusion, Orthodontic Treatment, and Orthognathic Surgery
 Short Face Growth Patterns: Maxillomandibular Deficiency
Short Face Growth Patterns: Maxillomandibular Deficiency
![]() Long Face Growth Patterns: Maxillary Vertical Excess with Mandibular Deformity
Long Face Growth Patterns: Maxillary Vertical Excess with Mandibular Deformity
![]() Primary Mandibular Deficiency Growth Patterns with or without Maxillary Arch Constriction
Primary Mandibular Deficiency Growth Patterns with or without Maxillary Arch Constriction
 Maxillary Deficiency with Relative Mandibular Excess Growth Patterns
Maxillary Deficiency with Relative Mandibular Excess Growth Patterns
 Syndromes with Craniosynostosis: Evaluation and Treatment
Syndromes with Craniosynostosis: Evaluation and Treatment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Aesthetic Alteration of the Soft Tissues of the Neck and Lower Face: Evaluation and Surgery
