By transferring volume from prominent eyelid fat pads to deficient midfacial hollows, fat transfer techniques utilized in lower blepharoplasty offer an effective method for aesthetically contouring the lid-cheek junction—an outcome not achievable with a purely subtractive approach. This article provides an anatomical foundation for the facial cosmetic surgeon performing aesthetic lower eyelid blepharoplasty in context of the aging midface. The application of adjacent fat transfer with both transconjunctival and transcutaneous approaches to lower blepharoplasty is outlined along with preoperative and postoperative considerations, complications, and guidelines for their avoidance.
Key points
- •
Understand anatomic basics and volumetric changes of the aging midface.
- •
Provide key preoperative considerations for adjacent fat transfer techniques.
- •
Discuss the application of adjacent fat transfer techniques and their utility within the various surgical approaches to lower eyelid blepharoplasty along with adjunctive procedures which facilitate a tailored approach to individual anatomy.
- •
Outline complications relevant to lower blepharoplasty with adjacent fat transfer and offer pearls for avoidance.
- •
Introduce a reference list for further in-depth study.
Introduction
In contemporary aesthetic lower blepharoplasty, there has been a trend towards:
- 1.
Volume preservation [ ], aimed at achieving more durable aesthetic outcomes by anticipating atrophic changes associated with aging, and thus minimizing the risk of eventual hollowing that may be noted with purely subtractive approaches [ ].
- 2.
Viewing the lower eyelid and midfacial transition as a single aesthetic unit, recognizing that successful rejuvenation requires addressing areas beyond the lower eyelid in isolation [ , , ].
These considerations have led to development of techniques directed at a transposition of excess orbital fat to fill, contour, and mask adjacent areas which are deficient in volume, such as the tear trough or palpebromalar groove to approximate a smooth, youthful transition to the midfacial region. A survey of ASOPRS surgeons found that 80% incorporate adjacent fat transfer in their approach to lower blepharoplasty [ ]. This article seeks to introduce the facial cosmetic surgeon to techniques in adjacent fat transfer as well as key considerations concerning their application in surgical midfacial rejuvenation.
Lower eyelid surgical anatomy
In performing blepharoplasty involving adjacent fat transfer techniques on the lower eyelids, a firm understanding of the pertinent anatomy and changes that occur with the aging midface is essential for minimizing complications, while maximizing anatomic and aesthetic success [ ].
With some individual variation, the lower eyelid margin has a gentle concave contour at the inferior corneal limbus, with its nadir just temporal to the midpupillary line ( Fig. 1 ) [ ]. The lower eyelid is divided into the anterior (skin and orbicularis oculi), middle (orbital septum), and posterior lamellae (eyelid retractors or capsulopalpebral fascia, tarsus, and palpebral conjunctiva).
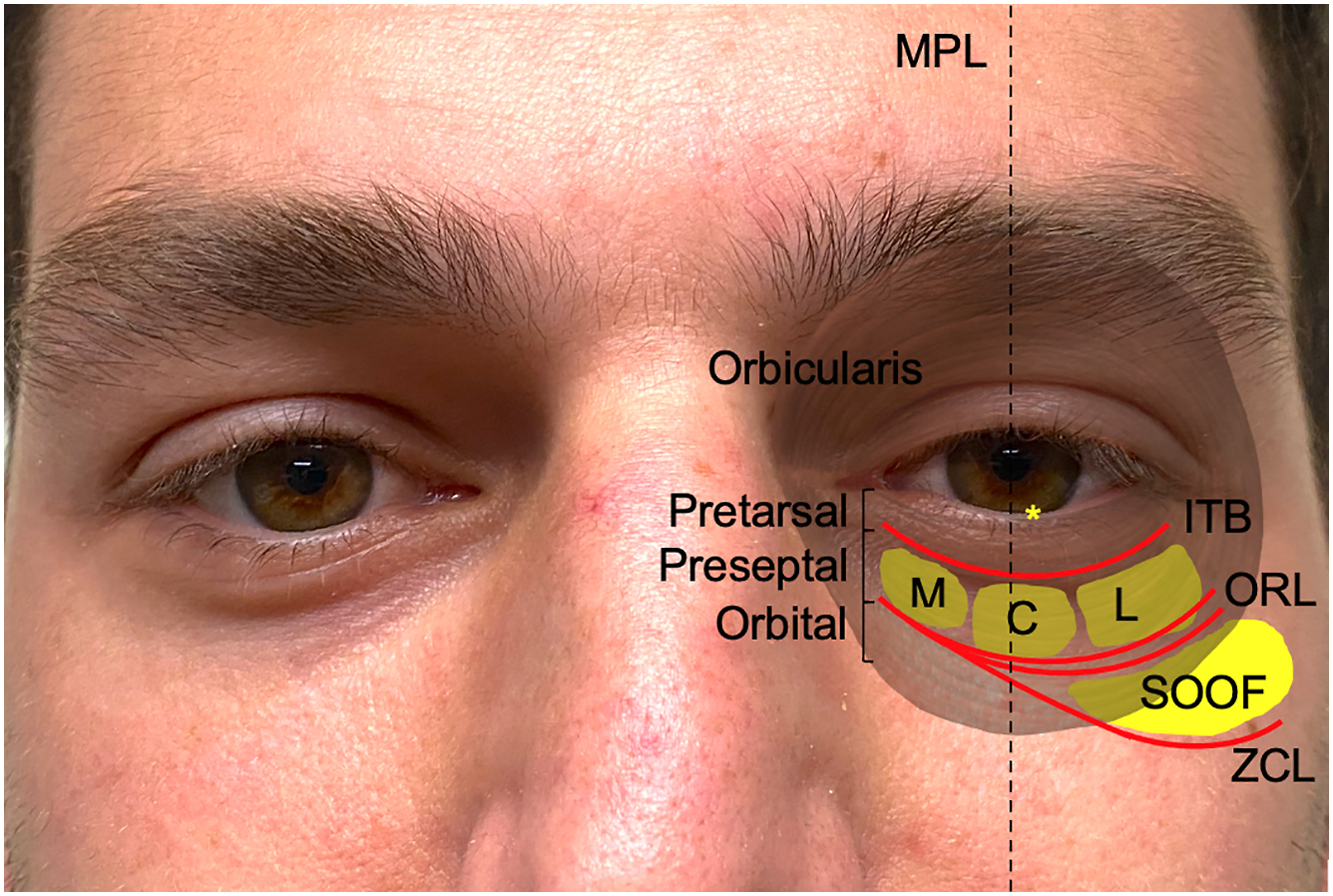
Apart from a subciliary prominence or “pretarsal roll”, which is formed by tonal contraction of the pretarsal orbicularis [ ], the lower eyelid volume is chiefly constituted by 3 retro-septal fat pads. The inferior oblique divides the medial and central fat pads [ ], while Clifford’s ligament, an arcuate expansion of Lockwood’s ligament extending from the retractors to the lateral infraorbital rim, divides the central and lateral fat pads [ ]. In addition to being a check ligament for the inferior rectus and inferior oblique, the arcuate expansion maintains lateral support to the eyelid by preventing backwards displacement of Lockwood’s ligament [ ]. The lateral fat pad may be subdivided into an anterior and posterior component, with the anterior portion extending over into the recess of Eisler where the orbital septum inserts 2 mm outside the inferolateral orbital rim [ ].
The lower eyelid is suspended by the bilaminar orbicularis (or orbital) retaining ligament (ORL, also orbitomalar ligament), which is continuous with the lateral orbital thickening laterally and the orbital septum superiorly [ ], and which indirectly secures the deep orbicularis and overlying skin to the orbital rim, providing major osteo-cutaneous support to the midface [ , , ]. The ORL also constitutes the superior border of the sub-orbicularis oculi fat (SOOF), which is deep to the orbital orbicularis and confined inferiorly by the zygomatico-cutaneous ligament [ ]. The lateral fibro-fatty SOOF is continuous with the inferior temporal compartment of the midface via the temporal tunnel, whereas its medial aspect extends 2 mm to 4 mm medial to the midpupillary line [ , ]. It provides a supportive buttress to the midface in addition to contributing to volume [ ]. These fatty and ligamentous structures within the youthful midface are depicted in Fig. 1 .
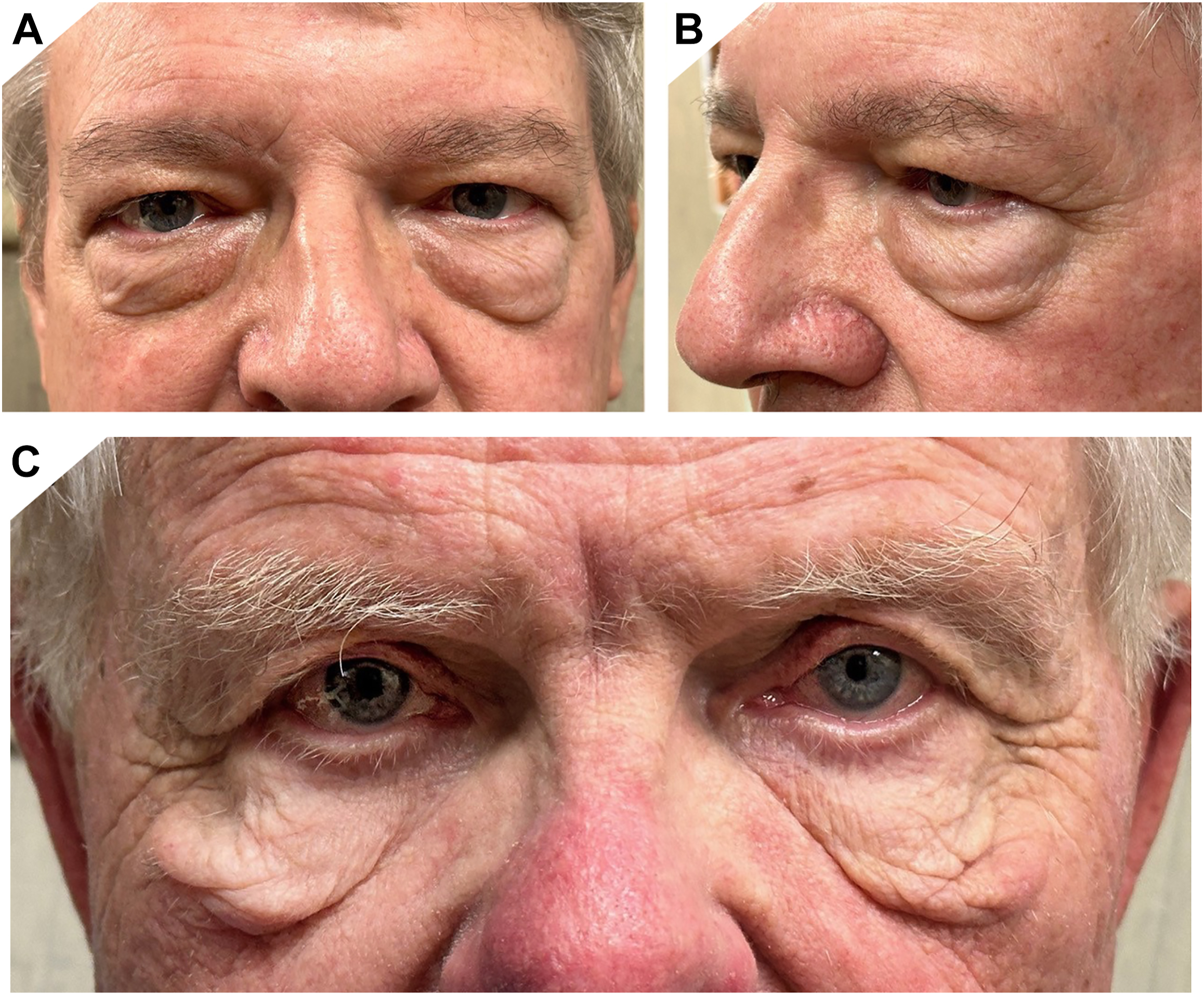
The undesirable appearance of “(under) eye bags”, or lower eyelid steatoblepharon, is due to herniation and/or expansion of the orbital fat pads against an attenuated orbital septum and orbicularis ( Fig. 3 ) [ , ]. Excessive steatoblepharon creates a step-off between palpebral and malar skin, expanding apparent eyelid height [ , ]. The development of dermatochalasis, hyperpigmentation, and rhytidosis also contributes to increased eyelid prominence [ , ]. These changes exacerbate the “tear trough deformity”, which Flowers attributed to poor development of the infraorbital malar complex, descent of aging malar tissues, volume loss of facial tissues, and a muscular defect between the inferomedial orbital orbicularis and levator labii superioris (angular head) [ ].
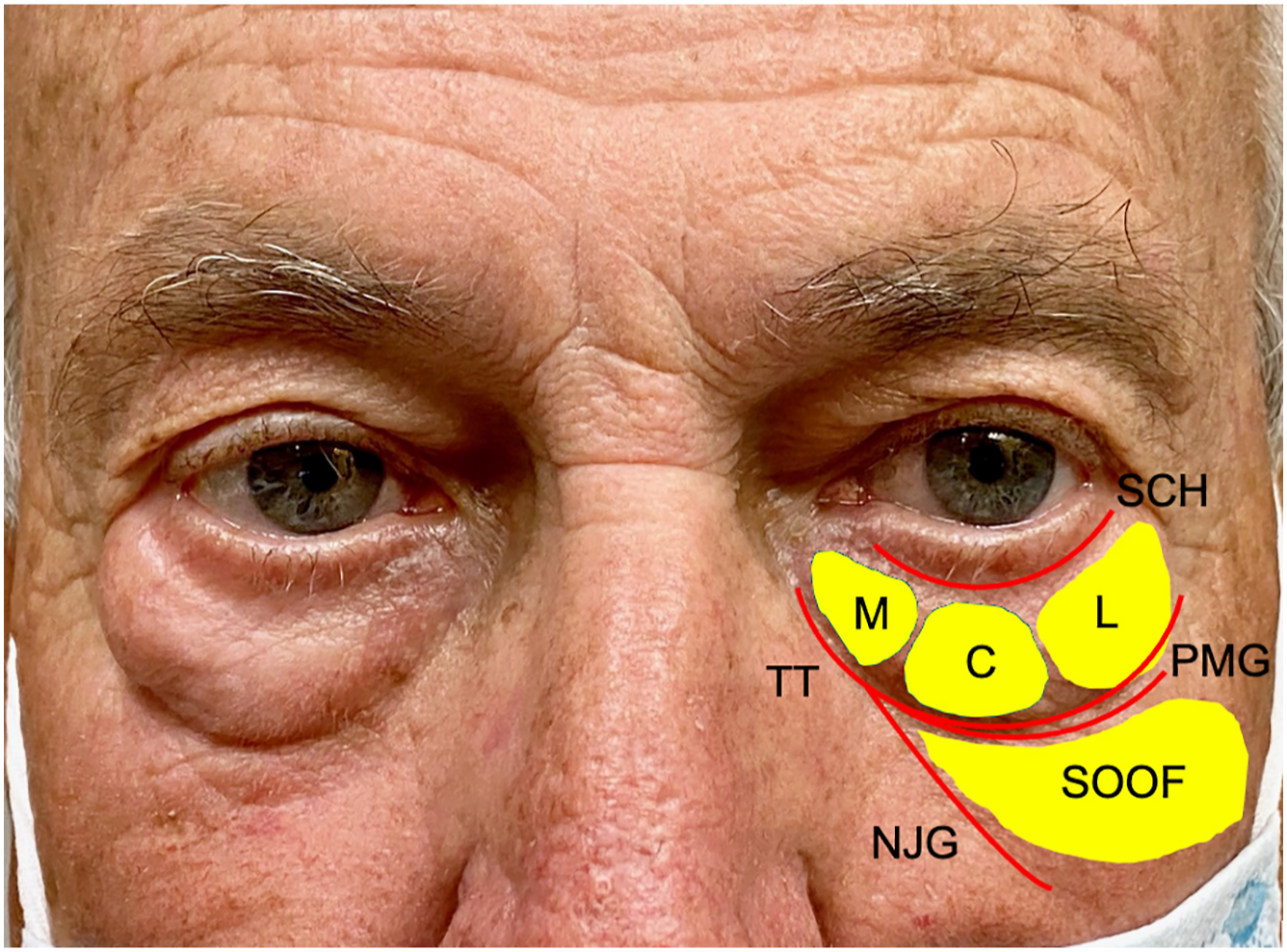
The orbital rim hollow is constituted medially by the tear trough hollow and laterally by the palpebromalar groove; it is bounded superiorly by the orbital fat pads and inferiorly by the SOOF and malar fat pads ( Fig. 2 ) [ ]. Other areas where there is close association of skin to underlying bony or ligamentous support similarly give rise to hollows that become more apparent as surrounding soft tissues age [ ]. Other hollows have been described around the orbital rim (see Fig. 2 ).
- 1.
Superiorly lies the septal confluence or eyelid crease hollow, formed by the convergence of the retractors, orbital septum, and tarsal plate [ , ].
- 2.
Inferiorly, the “nasojugal fold/groove” is found at the inferior orbital orbicularis and extends from the tear trough laterally at an oblique angle [ , ].
- 3.
The zygomatic hollow or “midcheek groove” overlies the medial zygomatico-cutaneous ligament and extends from the tear trough obliquely between the levator labii superioris and zygomatic muscles [ ].
These hollows and their intervening convexities or “mounds” often constitute a “double convex deformity” of the lower eyelid, wherein prolapsed orbital fat forms the superior convexity, a hollowed inferior orbital rim the concavity, and the malar mound the inferior convexity [ ].
A negative orbital vector occurs where inferior orbital rim is located more posteriorly than the cornea and is considered unaesthetic, giving the appearance of “bulging eyes” [ ]. Conversely, a positive orbital vector is associated with “deeper-set eyes”. Festoons—cascades of lax skin and orbital orbicularis sometimes also containing herniated fat and edema—may occur between orbicularis retaining and zygomatico-cutaneous ligaments [ ]. Their extent is always inferior to the orbital rim, as opposed to prominence of the fat pads above (see Fig. 3 ).
Preoperative considerations for adjacent fat transfer
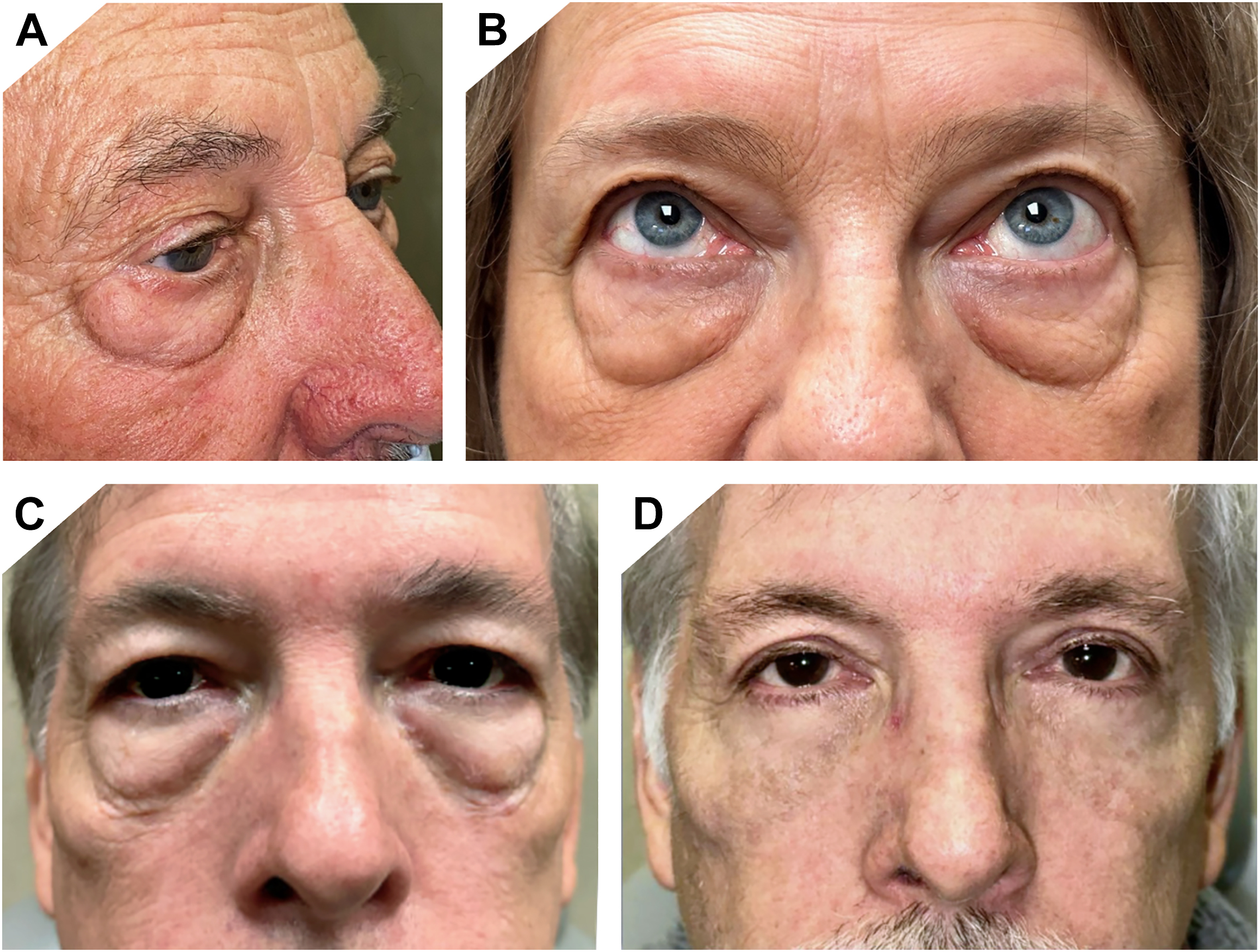
Each patient should be carefully evaluated to determine the best surgical approach—detailed preoperative assessment must consider ophthalmic and systemic history, including past surgical interventions, and involve individualized discussion of the expected outcomes and limitations of surgery. Reference photos are helpful in this regard, and comprehensive photographic documentation in standardized reference frames ( Fig. 4 A, B ) for both preoperative and postoperative states is critical ( Fig. 4 C,D) [ ]. Various grading systems have been proposed for the tear trough deformity ( Table 1 ) [ , , ] and steatoblepharon ( Table 2 ) [ , ]; these provide a helpful algorithmic basis for clinical assessment of patient eligibility for various lower blepharoplasty techniques.
| Grading/System | Description |
|---|---|
| Barton et al, [ ] 2004 | |
| Grade 0 | Absence of medial/lateral lines demarcating arcus marginalis/orbital rim; smooth, youthful contour without a transition zone at orbit-cheek junction |
| Grade I | Mild, subtle presence of a medial line or shadow; smooth lateral transition of orbit-cheek junction |
| Grade II | Moderate prominence of a visible demarcation of orbit-cheek junction, extending medial to lateral |
| Grade III | Severe demarcation of orbit-cheek junction; obvious step between orbit and cheek |
| Hirmand [ ] 2010 | |
| Class I | Volume loss limited medially to tear trough; may have mild flattening extending to central cheek |
| Class II | Volume loss in lateral infraorbital area in addition to medial orbit; may have moderate volume deficiency in medial cheek, flattening of central upper cheek |
| Class III | Full depression circumferentially along orbital rim; associated with more advanced volume deficiency in medial and central cheek, malar eminence |
| Sadick et al, [ ] 2007 a | |
| Tear trough depth | Each mm of depth=one point |
| Hyperpigmentation |
|
| Prolapse of nasal fat pad/pockets |
|
| Rhytidosis b |
|
a Sadick et al.’s tear trough rating score is the additive total of each component.
| Steatoblepharon grading | Description |
|---|---|
| +2 | Very prominent fat pads |
| +1 | Mildly noticeable fat pads |
| 0 | Absence of all 3 fat pads |
| −1 | Hollowing of periorbital fat |
The 2 main approaches for lower blepharoplasty are:
- 1.
Transconjunctival approach—avoids the potential for visible scars due to dissection from the posterior eyelid/conjunctival fornix.
- 2.
Transcutaneous approach—is performed through an external skin incision below the lash line. Whereas visibility may be better in this approach, iatrogenic orbicularis muscle injury can result in postoperative muscle atony, retraction, and ectropion [ ]. Many studies have also demonstrated a higher risk of lower eyelid malposition due to manipulation of the orbital septum [ ].
In a 2018 survey, the transconjunctival approach was more popular for lower blepharoplasty, utilized by 96% of respondents, versus 82% who employed the transcutaneous approach, 51% used both approaches [ ]. Although the transconjunctival approach is often preferred over the transcutaneous approach, both can afford excellent results for lower blepharoplasty with adjacent fat transfer when performed properly; thus individualization for each patient may warrant different techniques [ ].
Generally, young patients with minimal skin excess or textural changes would benefit from a transconjunctival approach, while older patients are more amenable to a transcutaneous approach to include excision of redundant skin [ ]. A combination of anterior and posterior approaches can also be performed, and in some cases, skin resurfacing with ablative lasers can replace skin excision and augment outcomes [ ].
Adjacent fat transfer techniques may be employed regardless of chosen approach to lower blepharoplasty, and are most applicable for patients in whom there is both steatoblepharon as well as hollowing at the tear trough and/or palpebromalar groove; in effect, volume may be borrowed from the former areas where it is in excess to fill in relative voids of the latter.
Subtractive lower blepharoplasty without fat transposition could be considered sparingly in young patients with isolated fat prominence and limited to no skin redundancy or midfacial ptosis [ , ]. In such patients, a transconjunctival incision avoids the potential for a visible scar; as the midface has not yet descended and exposed the inferior orbital rim, transposition of fat is less needed. However, for most patients, a purely subtractive approach can result in a hollowed or skeletonized appearance that may appear more aged, as it accentuates any shadows in the lower eyelids [ ]. This is particularly noticeable in patients with thinner skin, naturally dark shadows, or prominent lower eyelid vessels in whom removing additional fat through subtractive surgery can exacerbate the issue. In contrast, adding volume to the lower eyelid and over the orbital rim can improve the hollowed and shadowed appearance of the tear trough [ ].
The appearance of festoons can generally be improved through lower blepharoplasty with adjacent fat transfer, which is more forgiving than a purely subtractive approach in smoothing of the lid cheek junction. Ancillary procedures such as a midface lift or direct excision may be considered along with other noninvasive techniques including ablative laser resurfacing or chemical peels [ , ].
Cheek projection and vector of the orbital rim and malar eminence in relation to the anterior-most aspect of the cornea and lower eyelid margin should be noted, and the relative position of the ocular apex documented via exophthalmometry. A negative vector may require inferior orbital rim/malar augmentation, or additional vertical support to the lower eyelid with an implant in order to decrease risk of eyelid retraction following blepharoplasty [ ]. Distribution of fat across the inferior orbital rim during lower blepharoplasty may help augment volume where it is deficient and thereby improve the apparent orbital vector.
Eyelid margin malpositions such as ectropion or entropion should be considered when planning an approach to lower blepharoplasty as concurrent repair can enhance the aesthetic outcome and guard against complications such as lid retraction.
Relative contraindications for lower blepharoplasty with fat transposition include preexisting lower eyelid retraction and/or cicatricial change as well as excessive hollowing, suggesting insufficient orbital fat volume, in which case augmentation techniques rather than adjacent fat transfer should be considered. Absolute contraindications include inflammatory conditions of the orbit which involve the fatty tissues, such as active thyroid eye disease, which may complicate healing and increase risk of postoperative inflammation. Dry eye syndrome should be optimized prior to proceeding with surgery.
Surgical techniques
Lower eyelid blepharoplasty is safely performed under local anesthesia with oral sedatives or under monitored anesthesia. General anesthesia may be considered if excessive traction on fat pads is uncomfortable, if the patient is highly anxious, or if minimizing the volume of local analgesics to limit anatomic distortion is desired [ ].
Transconjunctival Approach
A mixture of 1% lidocaine and 0.25% bupivacaine with 1:100,000 epinephrine is injected into the inferior fornix, skin, and fat pads to ensure adequate anesthesia and hemostasis without excessive anatomic distortion. Conjunctiva is incised with Westcott scissors, monopolar cautery, or CO 2 laser in an arcuate fashion below the inferior tarsal border [ ]. Since the initial description of this approach by Bourguet in 1924 and its later popularization by Tessier [ , ], various modifications have led to 2 contemporary modes by which the infraorbital fat pads may be accessed:
- 1.
Preseptal (2 mm–4 mm inferior to the tarsus), which initiates the dissection plane anterior to the orbital septum, which is then opened over each fat pad ( Fig. 5 ).
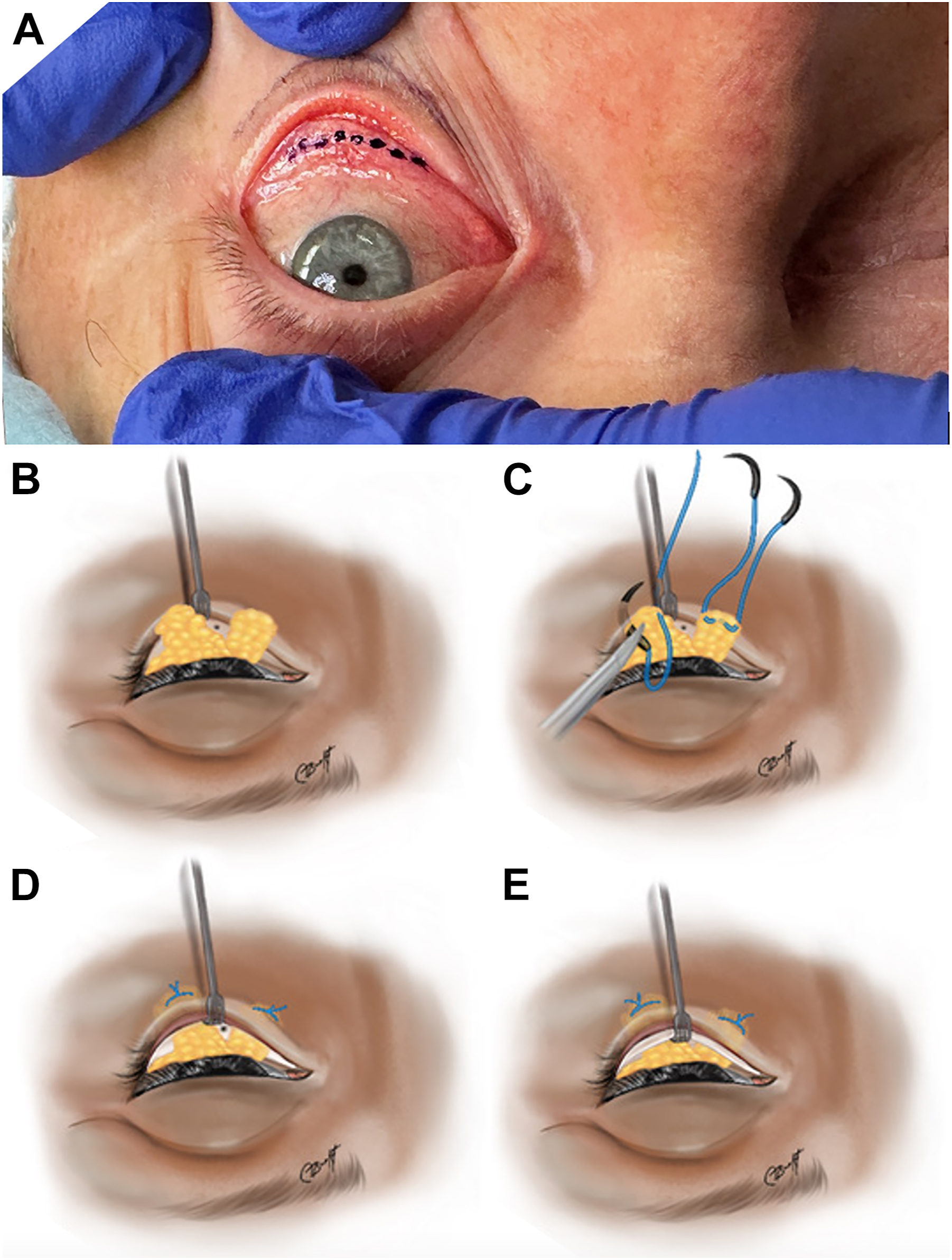
Fig. 5
Transconjunctival approach with fat repositioning. ( A ) Surgeon’s view of incisional marking approximately 2 mm inferior to the inferior border of the tarsus. Fat pads are dissected, fashioned into ( B ) pedicles and ( C ) loosely imbricated with polypropylene sutures, then transposed across the inferior orbital rim. ( D ) Preperiosteal fat repositioning is demonstrated with externalization of sutures below the tear trough, versus ( E ) a subperiosteal fat repositioning; the periosteum observed as a thin white layer.
( Illustrations by Cat N. Burkat, MD FACS . Data from [ , , , ].
- 2.
Postseptal (6 mm–7.5 mm inferior to the tarsus), which avoids violation of the septum by incising directly from the conjunctiva and retractors into the fat pads [ ].
Exposure of the forniceal space and fat pads may be enhanced with the use of a retractor (eg, Desmarres, Senn, or malleable) or traction sutures placed in the conjunctival/retractor layer pulled upwards over the globe (see Fig. 5 ) [ ]. Conjunctival pocket incisions should be avoided in favor of a longer continuous incision as they may limit visibility during fat repositioning.
Once accessed, gentle retropulsion of the globe prolapses the fat pads, which may be further exposed with forceps by light traction. During dissection, care must be taken to avoid disruption of the intervening inferior oblique muscle or arcuate expansion [ , ], though the latter is sometimes lysed to allow access to the posterior “Putterman” fat pad which can account for residual temporal fullness [ ]. The exposed fat pads can then be transposed to shift their volume to conceal undesired hollows with or without partial reduction.
Fat reduction
Often, some fat excision is necessary in shaping pedicles prior to transposition in facilitating optimal contour, though a minority of surgeons prefer to preserve all fat in performing a transposition [ ]. While the amount of excess fat varies in each patient, we prefer to utilize all of the fat when possible to optimally drape the entire medial to lateral orbital rim. Meticulous hemostasis during fat pad manipulation and before closure is critical to avoid retrobulbar hemorrhage. Cross-clamping with a hemostat in conjunction with application of cautery may be beneficial. Intermittent external inspection of the lower eyelid helps prevent excessive fat removal which would exacerbate a tear-trough hollow.
Fat repositioning
Fat pedicles are draped across the inferior orbital rim, reducing its prominence and providing a more youthful contour by smoothing the hollowed transition point (see Fig. 5 ) [ ]. The pedicles, either whole or sparingly reduced, are transposed over the inferior orbital rim into prezygomatic and premaxillary spaces created within one of a few midfacial dissection planes.
- 1.
Supraorbicularis plane (less commonly used): where pedicles are tucked in between skin and orbicularis [ , ].
- 2.
Suborbicularis plane: where fat is tucked into a pocket fashioned below the orbital orbicularis. While posing a higher risk of injury to vascular structures, it allows more direct access to release the ORL and arcus marginalis, providing access into premaxillary and prezygomatic spaces, which is useful in correcting contour issues of the tear trough and lid-cheek junction [ , ].
- 3.
Preperiosteal/intra-SOOF plane: where fat pedicles are thought to thrive from placement adjacent to, or within, the SOOF due to the vascularity of this space [ ]. Though denervation of the orbicularis (whose terminal innervation rises through SOOF) and resulting ectropion can be a concern [ ], this complication may be avoided by a limited dissection 8 mm to 12 mm below the inferior orbital rim and away from the “critical zone”, a circular area of 0.5 cm radius, with its center located 2.5 cm inferolateral 30° to the lateral canthus [ ].
- 4.
Subperiosteal plane: accessed by incision of the arcus marginalis below inferior orbital rim, followed by elevation of periosteum via Freer or Cottle elevator to fashion a pocket extending approximately 15 mm inferiorly. While potentially providing better outcomes relating to contour and postoperative edema/ecchymosis as it is a relatively avascular plane, it risks disrupting the infraorbital nerve [ , , ].
Studies have demonstrated similar aesthetic results with either supra or sub-periosteal fat transpositioning [ ].
An ORL release may be performed in conjunction within any of the above dissection planes. Either a monolamellar or bilamellar lysis may be performed depending on the extent of the tear trough deformity as suggested by Rohrich and colleagues [ ]. With one of a variety of instruments such as monopolar cautery, scalpel, or CO 2 laser, the ligamentous attachment of the ORL is first incised, and the ligamentous attachments released proceeding from medial to lateral with a Freer or Cottle elevator [ , ]. Dissection should be caried out within a “safe zone” described by Choi and Kim as bounded 9.4 mm from medial canthus line, 3 mm from the lateral canthal crease, and 6.0 mm from the eyelid margin to avoid damage to the palpebral branch trunks where they cross the orbital rim [ , ]. It is recommended that if electrocautery is used in dissection, the device tip should be directed deeper toward the bone (rather than parallel to the skin surface) to limit exposure of nervous tissue to injury from radiant heat [ ].
It is critical to release all septal attachments from the base of the fat pedicle in order to avoid lower eyelid traction. The fat pedicle should be freely mobile with absolutely no lower eyelid pulling when the fat is transposed inferiorly. Pedicles can be transposed directly over the orbital rim or shifted medially or laterally as needed to volumize any areas of deficiency; placement within each individual eyelid may vary depending on the specific areas of volume deficiency, and according to how eyelid-midface contour might best be improved. The fat pads may also be variably debulked or excised prior to transposition as pedicles. Most surgeons also prefer debulking the lateral fat pad, while repositioning only the medial and central pads. Others may transpose all 3: for instance, one fat pedicle can be draped over the medial-most orbital rim, another placed inferiorly and medial to the infraorbital foramen, with the final fat pedicle directed laterally. By transposing multiple pedicles in different vectors, optimal effacement can be achieved.
Fat pedicles are secured to their desired location with sutures via external, internal, or combined methods of fixation (see Fig. 5 ) [ , , ].
- •
In external fixation, sutures are typically placed temporarily; they are first introduced through the skin at a point below the ORL into a sub-orbicularis/sub-periosteal pocket, then engaged apically through the fat pedicle and returned full thickness through skin to quilt it into place [ , , ]. Alternatively, a double-armed suture allows both needles to travel from pedicle to skin, thus only passing away from the globe.
- •
With internal fixation techniques, transposed fat is either secured subcutaneously or to other structures within the dissection plane, such as periosteum [ , ].
- •
As there is some thought that transposed fat is prone to retract back into the orbit, combination internal/external fixation may be used to provide a dual means of secure fixation [ ].
As exposure via the transconjunctival approach is often limited, especially with tight eyelids, a small needle is recommended. The use of permanent sutures, which are removed the following week, is favored by the authors due to their lower potential to cause an inflammatory reaction, or cyst, or granuloma formation.
Fat transposition may be performed even in patients without excess infraorbital fat, such as those who have had prior reduction, or in younger patients, so long as there is sufficient fat volume present [ ]. The interposition of a fatty spacer over the orbital rim, whether it be a fat pedicle or free fat graft introduced from another site (such as concurrent upper blepharoplasty or face lift) is thought to permit sustained effacement of the tear trough deformity by preventing readherence of released ligaments [ , ]. The long-term durability of transposition techniques has yet to be conclusively determined in the literature [ ].
At closure, some surgeons may prefer securing the retractor layer and/or conjunctiva with 1 to 2 fine sutures such as 6-0 (fast, plain, or chromic) gut or 7-0 polyglactin; buried placement minimizes postoperative discomfort. It is also acceptable for the incised conjunctival edges to simply be apposed to avoid overlapping without suture closure. While a sutureless method confers the benefit of providing an outlet of any fluid buildup, it also permits entry of foreign materials such as ointment or ophthalmic lubricant [ ]. We typically place 1 to 2 sutures to close the inferior retractor layer only. Instructions for the application of topical ointments such as erythromycin, tobramycin, or neomycin-polymyxin-dexamethasone should be reviewed.
Transcutaneous Approach
Skin marking
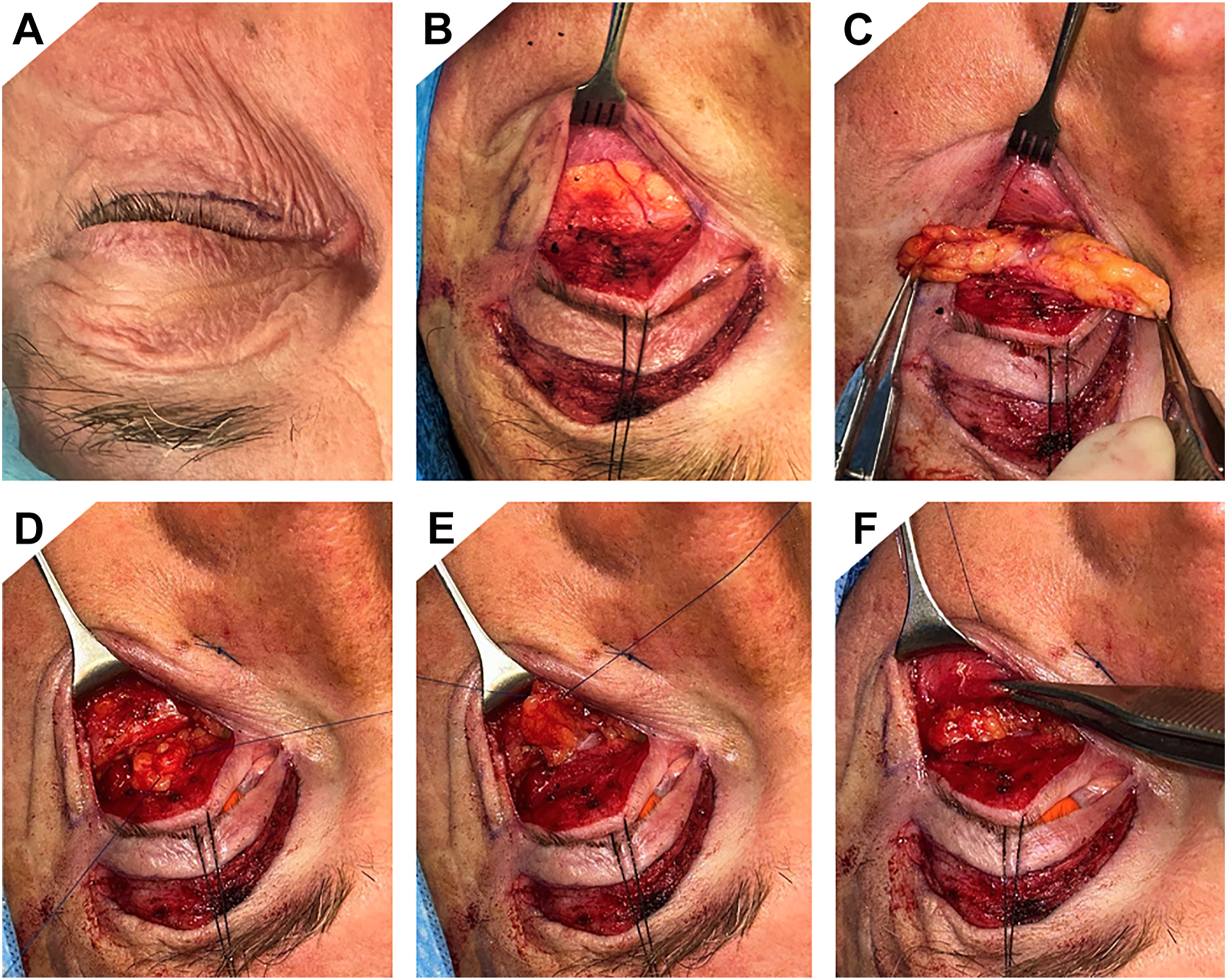
Transcutaneous lower eyelid blepharoplasty is performed through a subciliary incision about 1 mm to 2 mm below the lash line extending 4 mm to 5 mm from the lateral canthus ( Fig. 6 ) following administration of local anesthetic to the skin, orbicularis, and fat pads [ ].
Related posts:
 Update on Anesthesia and Pain Management Strategies in Cosmetic Surgery
Update on Anesthesia and Pain Management Strategies in Cosmetic Surgery
 Body Contouring After Massive Weight Loss
Body Contouring After Massive Weight Loss
 Endpoints in Laser & Light-Based Devices
Endpoints in Laser & Light-Based Devices
 Adjustments to the Maxillofacial Skeleton to Improve Facial Harmony
Adjustments to the Maxillofacial Skeleton to Improve Facial Harmony
 Filler Rhinoplasty
Filler Rhinoplasty
 Whitnall’s Ligament Suspension Repair of Involutional Ptosis—The Old Is New
Whitnall’s Ligament Suspension Repair of Involutional Ptosis—The Old Is New
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


