The complexity of the midface structure and its importance to a multitude of functions present the reconstructive surgeon with unique challenges. The midface is an area that is crucial both functionally and esthetically. Midface reconstructions can make profound differences in form and function. This review focuses on complex midface and maxillary reconstructions requiring free tissue transfer.
Key points
- •
Midface reconstruction is complex due to its importance functionally and esthetically and the intricacies of the anatomy.
- •
The reconstructive surgeon will select the free flap donor site best able to account for the size of the defect, the buttress(es) lost, the functional needs, and esthetic goals.
- •
Innovations in virtual surgical planning allow for greater accuracy and applicability of the technology.
- •
Further research is warranted as current studies evaluating outcomes of midface reconstruction are heterogenous and lack a standardized reporting of esthetic or functional outcomes.
Introduction
The midface, or middle third of the face, includes the malar, zygomatic, and orbital areas. The midface is involved in facial expression, speech, and mastication. In addition, it is an important component of facial esthetics. This coupled with its complex three-dimensional (3D) structure results in a challenging area to reconstruct. There are 6 pairs of bones (nasal, maxilla, palatine, lacrimal, zygoma, and inferior nasal concha) that provide a framework for the midface. The majority of the boney framework is supported by the zygoma and maxilla. The facial skeleton and the overlying soft tissues are responsible for the projection in this region, an important component of facial esthetics. The goals of midface reconstruction depend on the defect and may include any combination of the following: closures of a fistula, restoration of soft tissue volumetric loss and symmetry, prevention of velopharyngeal insufficiency, orbital positioning, dental rehabilitation, and restoration of a bony framework for function and soft tissue support.
Following the introduction of microvascular free flap (FF) reconstructions for head and neck defects in the 1990s, there has been significant innovation in the realm of midface reconstruction. Prior to the availability of FFs, the primary reconstructive option for patients with a midface defect was an obturator. , Several publications have reported improved functional and cosmetic outcomes with FF reconstruction of a midface defect when compared to an obturator. These included improved quality of life, reduction in pain, greater mastication efficiency, improved speech intelligibility, and reduced levels of anxiety. ,
Currently, there is a wide variety of reconstructive options for midface reconstruction, each with their own advantages and disadvantages. These range from prosthesis and obturators to local and pedicled flaps and finally microvascular FFs. Often, the integration of several techniques is required to optimize the outcomes for patients. In this review, we will discuss advanced midface reconstruction including challenges and new innovations.
Considerations
Given the complexity of midface anatomy, it is not surprising that several classification systems exist. While the most referenced is the Brown classification system described in 2010, there is currently no standard in the reporting of outcomes for midface reconstruction. The Brown classification system ( Table 1 ) includes a grade for the vertical (isolated palate to orbital rim; classes I–IV) and the horizontal (extent of palate and alveolar ridge; a–c) aspect of the defect. The classification was modified later to include class V (orbitomaxillary, no palate or alveolus) and class VI (nasomaxillary, no palate or alveolus). One challenge with any midface classification system is the complexity of the defects often preclude them from fitting nicely into a single class. , Still, the reconstructive surgeon may find a classification system useful for conceptualizing the reconstructive needs based on what has been lost. While it does not currently exist, it has been proposed that the ideal midface classification would incorporate: (1) dental status, (2) presence of an oroantral or nasal cutaneous communication, (3) soft palate involvement, (4) vertical extent, (5) horizonal extent (medial–lateral), and (6) anterior-posterior extent. ,
| Vertical | Horizontal | ||
|---|---|---|---|
| I | Maxillectomy without oral or antral communication | a | Limited palate defect, alveolus intact |
| II | Inferior maxillectomy without resection of the orbital floor | b | Less than or equal to half of the palate resected on one side |
| III | Superior and inferior maxillectomy including resection of the orbital floor and periorbital | c | Bilateral hard palate and alveolus resection (equal to or less than half) or anterior hard palate and alveolus |
| IV | Extensive maxillectomy including resection of the orbit and possible skull base resection | d | Greater than half of the hard palate and alveolus resected |
| V | Superior maxillectomy including resection of the orbit | — | — |
| VI | Central maxillectomy including resection of the nasal aperture | — | — |
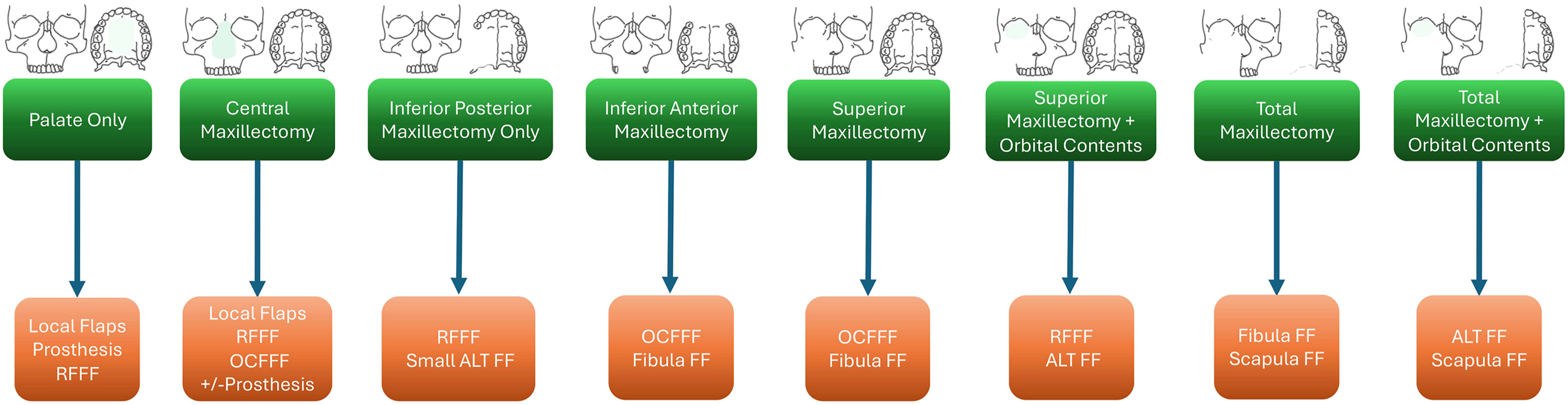
Terminology often used by surgeons to describe the extent of the maxillectomy performed includes medial, infrastructure, superstructure, subtotal, and total. A medial maxillectomy includes the removal of the medial wall of the maxilla adjacent to the nasal passage with the preservation of the hard palate and orbit. An infrastructure maxillectomy includes the removal of the hard palate and inferior portion of the maxilla including the teeth with the preservation of the orbital floor. A suprastructure maxillectomy includes the removal of the superior portion of the maxilla and the removal of the orbital floor with the preservation of the hard palate. A subtotal maxillectomy includes removal of a combination of the components the maxilla without removal of the entire maxilla. A total maxillectomy includes the removal of the entire maxilla including the hard palate and orbital floor. An algorithm of possible reconstructive options by defect is provided in Fig. 1 . While this may serve as a guide, it is important for the reconstructive surgeon to be aware that, in reality, these defects are highly variable and require a patient-specific approach. An in-depth understanding of the anatomy is crucial to achieving the desired outcomes.
Indications and goals
The defect assessment and goals of reconstruction will help guide the reconstructive surgeon both in surgical planning and donor site selection. Replacement of the lost bone is important to limit contracture and improve facial contouring. In addition, the volume of soft tissue lost must also be taken into consideration when selecting a donor site. Careful deliberation of the advantages and disadvantages of each donor site is critical.
To provide the framework and stability for the reconstructed midface, the restoration of any lost buttresses is paramount. This is most successfully achieved with a boney reconstruction. The roof (inferior orbital rims and zygoma) and floor (hard palate) of the midface make up the horizontal buttresses. While the nasomaxillary, zygomaticomaxillary, and pterygomaxillary make up the vertical buttresses of the midface. The framework for the maxillary dentition is the maxillary alveolus and nasal support is from the premaxilla.
Advantages and disadvantages
Careful consideration and planning are performed prior to the surgery. The reconstructive surgeon will weigh the advantages and disadvantages of each donor site to maximize the number of goals achieved. Reconstruction of a small ostial midface defects or single buttress may be achieved with the osteocutaneous radial forearm FF. While defects that involve numerous buttresses often require longer bone stock, making the fibula or scapula a more likely choice. If the maxillary alveolus is involved, dental rehabilitation is factored in when selecting a donor site. Dental implantation is possible with either a fibula or scapula FFs.
The infraorbital curvature has important esthetics implications and is difficult to reproduce with any donor site. In order to recreate this curvature and provide orbital support, there has been continued innovation with custom orbital floor implants. , These are often used with the addition of a soft tissue FF for coverage and protection of the implant from exposure to bacteria. Soft tissue donor sites commonly used include the anterior lateral thigh or radial forearm, depending on volumetric needs. Overlying skin breakdown, fistula formation, and extrusion of hardware are complications that can occur.
The radial forearm free flap (RFFF) is a fasciocutaneous flap that has proven useful in head and neck reconstruction due to his pliability, long pedicle length, and reliability. The long pedicle length is, particularly, advantageous for midface reconstruction in that it allows for tension-free anastomosis in the neck. The pedicle may also be harvested with additional adipose as needed for further volumetric contouring. Reconstruction of simple ostial midface defects may be achieved with the osteocutaneous radial forearm free flap (OCRFFF), and its ideal use includes defects limited to the alveolar ridge, infrastructure maxilla, or orbital rim. Limitations of the OCRFFF include limited bone length (10–12 cm), limited soft tissue volume, and lack of bicortical bone stock for dental implant integration.
The anterolateral thigh (ALT) FF is primarily chosen when large volumes of soft tissue loss are anticipated. Examples include large resections with orbital exenteration or when soft tissue is needed to either obliterate the sinus cavities or reinforce a skull base repair. It can also be utilized to provide coverage of custom-made orbital rim implants in the setting of an orbital rim reconstruction. Often, the ALT has greater subcutaneous adipose thickness when compared to the RFFF and subsequently may provide greater plate coverage and a lower incidence of hardware exposure. However, there is a great variability among patients in the thickness of the adipose and this should be taken into account.
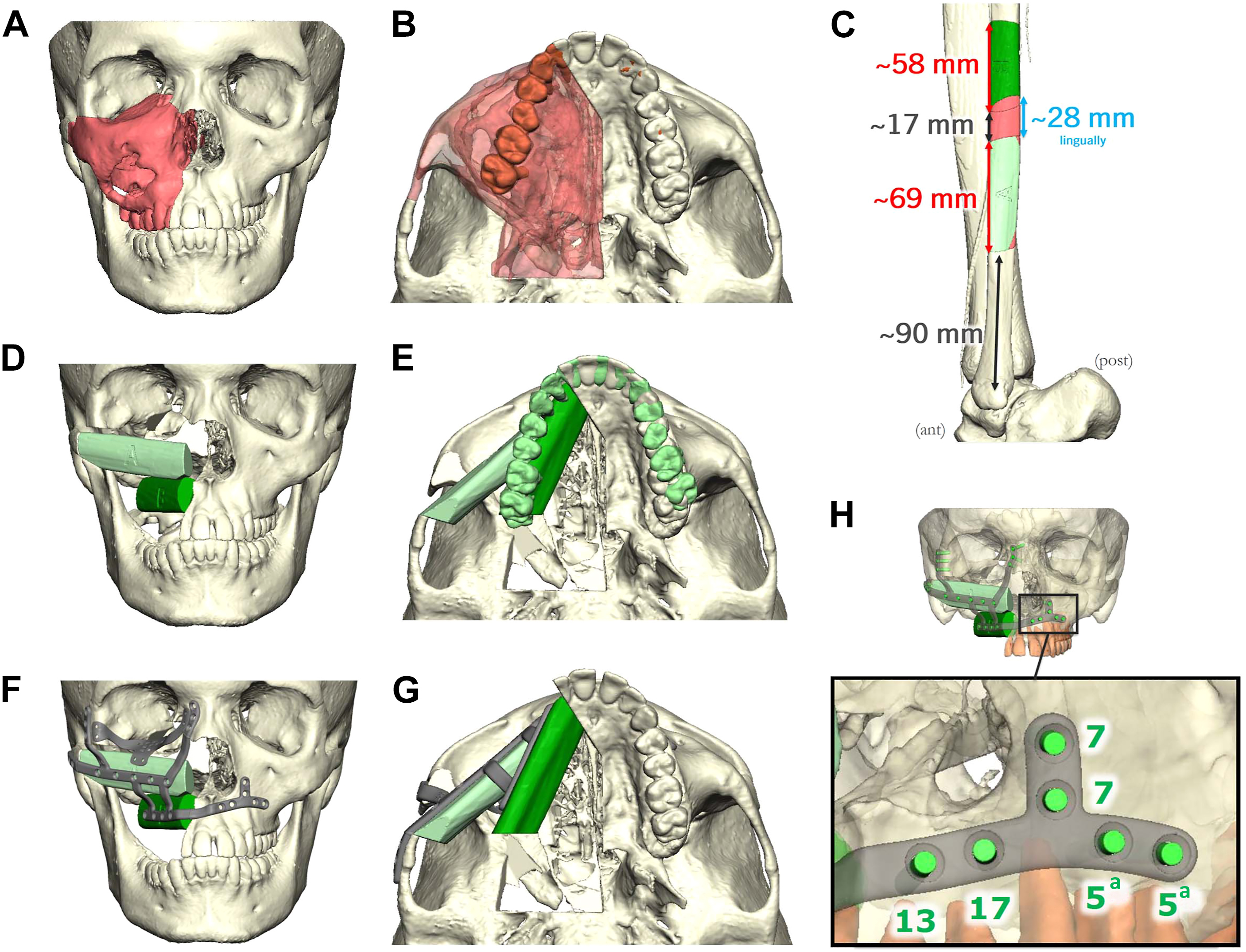
The bone stock provided by the fibula lends itself to great versatility for midface reconstruction. Multiple osteotomies can be made to improve restoration of the facial skeleton and contouring ( Fig. 2 ). The skin paddle is thin and pliable, which lends itself to increased versatility. Dental implantation is possible with the fibula bone due to the thickness and bicortical harvest. It is important to determine the length of bone and number of osteotomies required to achieve the reconstructive goals. The pedicle length will be reduced with each additional segment of bone. In addition, when segments are stacked to improve facial contouring, additional spacing along the pedicle is required between boney segments. This is known as the “leash” and helps protect the pedicle from kinking. These variables are of greater importance in midface reconstruction, which requires a longer pedicle length to reach the vessels in the neck. For example, a 3 buttress defect is less ideal for a fibula FF due to the length of bone needed and the number of osteotomies required.
Related posts:
 Microvascular Free Flap Practice Management and Career Development
Updates in Assisted Advanced Technology for Microvascular Free Tissue Transfer in Head and Neck Surgery
Contemporary Approaches to Head and Neck Reconstruction
Free Flap Reconstruction of the Oropharynx
Microvascular Free Flap Practice Management and Career Development
Updates in Assisted Advanced Technology for Microvascular Free Tissue Transfer in Head and Neck Surgery
Contemporary Approaches to Head and Neck Reconstruction
Free Flap Reconstruction of the Oropharynx
 Free Flap Enhanced Recovery Protocols in Head and Neck Surgery
Free Flap Enhanced Recovery Protocols in Head and Neck Surgery
 The Pinch Blepharoplasty
The Pinch Blepharoplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


