Microsurgical Advances in Extremity Salvage
Keywords
• Complex extremity injury • Free flap • Timing of reconstruction • Microsurgical extremity salvage
Introduction
During the past 40 years, evolution in reconstructive microsurgery has substantially influenced limb salvage surgery. Despite continuous improvement in trauma management leading to a significant reduction in primary limb amputations, complex injuries involving extremities remain a particular challenge for reconstructive surgeons. In the past, limb salvage procedures were often impended by local tissue status; modern methods of microsurgical free tissue transfer now allow an early, “custom-fit” wound management, aimed to optimally meet the individual functional and esthetic requirements of the affected trauma region. State-of-the-art reconstructive microsurgery has opened a wide range of possibilities in limb salvage surgery allowing immediate fracture and soft tissue repair with only minimal compromise in functional outcome. Key steps in surgical management include radical tissue debridement, adequate fracture stabilization, and reconstruction of viable structures (if necessary, by use of autologous blood vessels or nerve grafts). Subsequently, tissue defects should be covered by sufficient well-vascularized tissue, optimally matched to meet the individual tissue requirements at the recipient site.1 The authors outline the impact of recent microsurgical advances on extremity salvage and reconstruction.
Initial preoperative assessment
Initial stabilization and diagnosis should be performed via a multidisciplinary approach according to the established Advanced trauma life support protocol.2 For extremity trauma, immediate attention primarily targets hemorrhage control. Once the patient is stabilized, a focused clinical evaluation is performed. Assessment of injured extremities must consider trauma mechanisms, wound dimensions, and all functional components (soft tissue, nerves, vessels, and bones). These components must be examined individually and in combination.
Indications for reconstruction versus amputation
Indications for limb salvage procedures versus primary amputation must be evaluated individually for each patient, considering not only local trauma site but also patient age, presence of other concomitant injuries, patient comorbidities, patient socioeconomic status, and patient motivation. Despite major advancements in reconstructive microsurgery, severe lower extremity trauma (Gustilo IIIB-IIIC) is still associated with amputation rates of up to 40%.3,4 In general, indications for microsurgical free flap reconstruction include the following5:
The most commonly used classification system for lower extremity trauma has been the Gustilo classification, introduced in 1976 and subsequently modified in 1984 (Table 1). This classification analyzes not only wound dimensions and the presence or absence of neurovascular injury but also wound contamination and trauma energy impact.6
Table 1 Gustilo classification
| Gustilo Classification | Definition |
|---|---|
| Type I | Wound <1 cm, minimal contamination, low-energy and simple fracture |
| Type II | Laceration >1 cm; moderate soft tissue damage with adequate bone coverage |
| Type IIIA | Extensive soft tissue damage, massive contamination but adequate bone coverage |
| Type IIIB | Extensive soft tissue damage with periosteal stripping and bone exposure, flap coverage is usually required |
| Type IIIC | Arterial injury associated and requiring repair |
Numerous algorithms have been established, designed to estimate the viability of damaged tissue and to assist in determining whether amputation is necessary or whether limb salvage of traumatized extremities is recommended and promising. These include the Mangled Extremity Severity Score, the Limb Salvage Index, the Predictive Salvage Index, and the Hannover Fracture Scale.7–11 Besides providing an analysis of local tissue status, these scores also specifically consider arterial and venous vascular injury as a prognostic factor and warm ischemia and shock time. A prospective evaluation of 556 consecutive patients from 2001 on showed that, because of high specificity, low scores reliably predicted limb salvage potential. In contrast, because of low sensitivity, trauma evaluation scores did not reliably identify patients possibly requiring an amputation.12 Current data suggest that these scores can be useful tools in the decision-making process (when used cautiously). They should not be used as the principal means for reaching difficult decisions.13 From an economic point of view, unless amputation is inevitable, surgeons should always consider limb salvage, which will yields lower costs and higher utility compared with amputation.14
Special attention must be paid to complete traumatic limb amputation. If the patient’s life is at stake, the principle of “life before limb” will obviously be the primary objective. In this case, immediate replantation remains fairly uncommon.15 Indications for primary amputation may include advanced patient age, severe crush injuries with complete transsection of essential anatomic structures, prolonged warm ischemia time, or presence of potentially life-threatening concomitant injuries. In the case of traumatic amputation, warm ischemia can be tolerated up to 8 hours and cooling may extend the time-frame for replantation to 24 hours.16,17 A study published in 2005 demonstrated that plantar sensation is no longer a limiting prognostic factor when evaluating possible limb salvage, because it showed comparable functional outcomes in plantar sensation between patients initially lacking and patients with permanently preserved plantar sensitivity.18
Thus, a surgeon must perform realistic risk-benefit stratification to determine whether amputation is justified. When considering salvage procedures, expectations must be tempered by a realistic assessment of potential outcome, because protracted attempts for limb salvage may have a negative impact on the patient’s social, physiologic and psychological subsistence.19 In some cases, limb amputation may even be the preferable strategy because it may reduce the duration of hospitalization and rehabilitation. Several studies even suggest that patients with primary amputation show equally good functional outcomes as those who underwent limb reconstruction.20 The lower extremity assessment project demonstrated reconstruction results in 2-year outcomes equivalent to those of amputation.20
Timing
Since Marco Godina introduced the concept of the “emergency” free tissue transfer in the 1980s, surgical treatment of severe tissue trauma has experienced a substantial change.21 Early, fastidious trauma zone debridement followed by immediate restoration of affected longitudinal structures and early defect coverage by transferring adequately vascularized tissue has proved to reduce the incidence of osteomyelitis and fracture nonunion. In his study from 1986, Godina showed that delayed microsurgical reconstruction following trauma (between 72 hours and 90 days) was associated with the highest risk of infection and flap loss. Thus, he proposed the concept of “early” microsurgical reconstruction within 72 hours after trauma. Despite the proved advantage, the optimal timing for free tissue wound coverage remains controversial. Several consecutive studies analyzing the correlation between time until reconstruction and complication rate or functional outcome proved to be consistent with Godina’s initial results, showing that early microsurgical reconstruction significantly reduced bone union time, number of surgical procedures, and infection rate.22–25 In contrast, a study from 2008 showed no potential disadvantage associated with delayed lower extremity reconstruction.26 Byrd and colleagues22 demonstrated the importance of early soft tissue coverage after removing all devitalized tissue, thereby preventing bacterial colonization. Complex and contaminated wounds should be converted into surgically clean wounds to allow primary closure.24
There remains a wide and misleading variety of terms used for defining windows during which posttraumatic free flap wound closure is recommended. To reliably compare reconstructive results between individual institutions, a standardized terminology for the timing of free flap coverage is essential. Thus, Ninkovic and colleagues implemented a simple and versatile terminology, analogous to the established nomenclature defining the phases of normal wound healing.27
According to this terminology, flap closure timing is subdivided into 3 categories:
Primary flap cover for crucial closure prevents further tissue damage caused by desiccation and facilitates vascular ingrowth from the new surrounding soft tissue. Well-vascularized muscle free flaps provide healthy tissue, thereby allowing a radical debridement of the trauma zone. Because the primary goal in the treatment of complex extremity injury is a quick and functionally optimal recovery, the treatment of choice is the primarily free flap cover within the first 24 hours after injury. This minimizes morbidity, tissue infection rate, requirement for secondary surgical procedures, rehabilitation time, and total duration of hospital stay.28
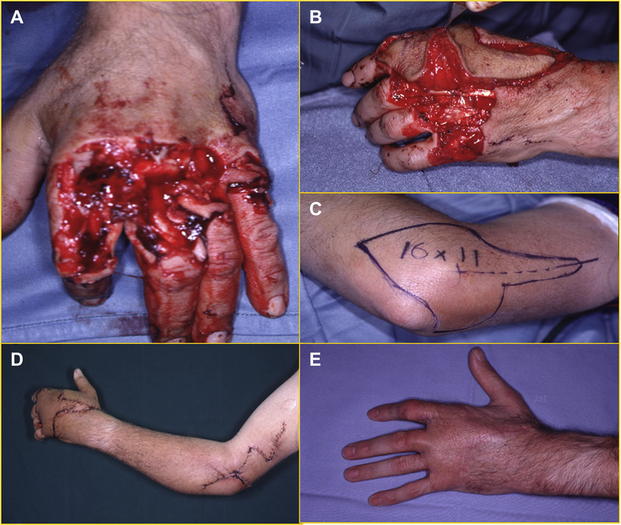
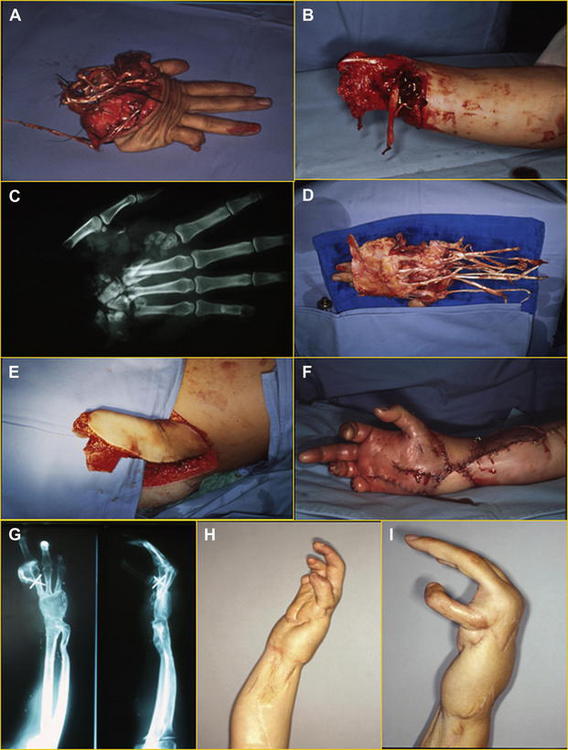
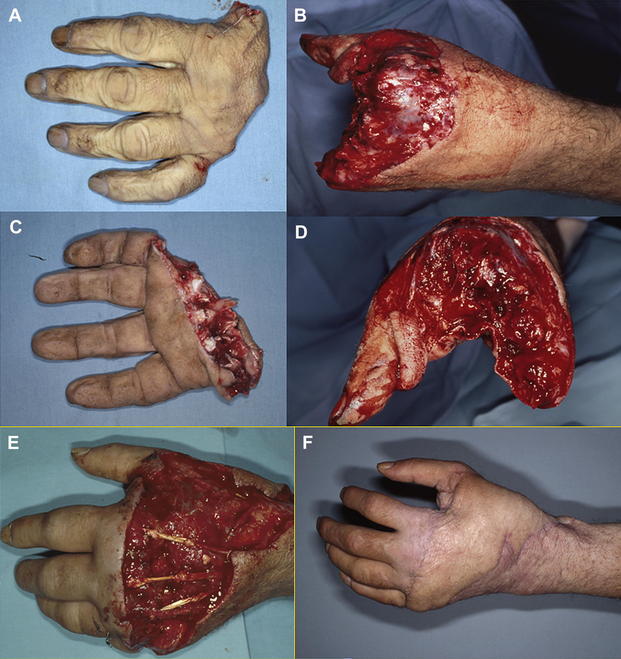
Primary free flap closure with primary reconstruction is defined as a combination of definite functional reconstruction of longitudinal structures (bone, vessels, nerves, and tendons using grafts if it is necessary) combined with free or pedicled flap coverage following surgical debridement as a single-step procedure within a period of 24 hours (Figs. 1 and 2).
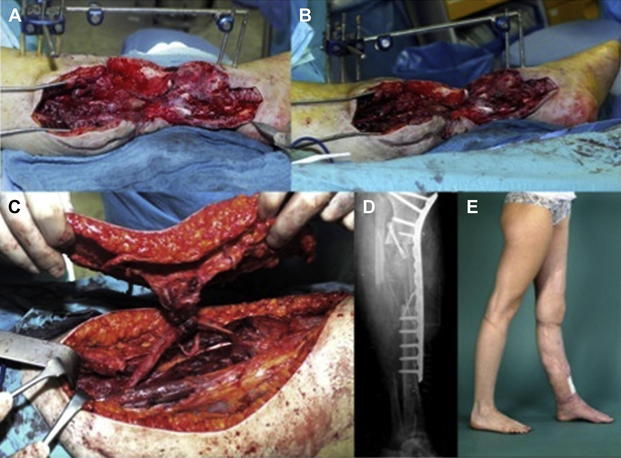
Delayed primary reconstruction is defined by free flap defect closure within 2 to 7 days after the trauma. Again, definite reconstruction of longitudinal structures can be performed within this time frame or later according to the wound condition and type of injury. It is important to consider that by delaying timing of definite defect closure, surgical options for reconstruction of longitudinal structures are significantly reduced without possibilities to replace the missing structure (eg, bone, tendon, nerve) with graft because of a higher rate of infection. However, this coverage allows the possibility of starting immediate physical medicine and, soon, definitive secondary reconstruction (Figs. 3 and 4).
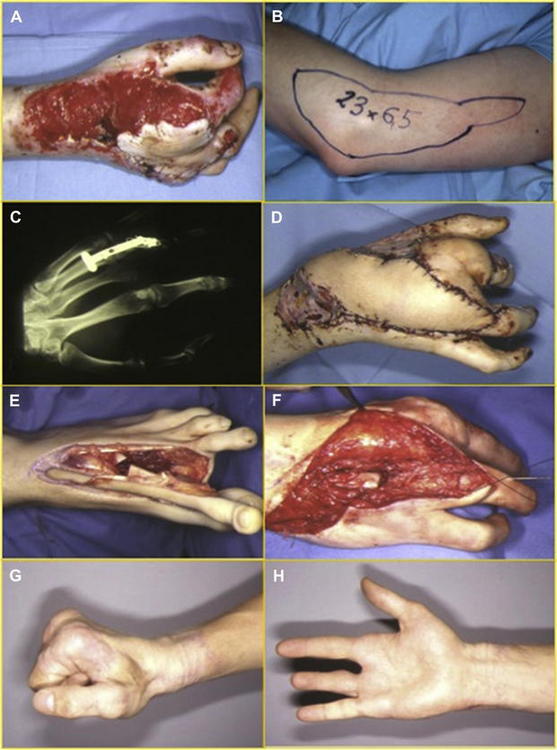
Secondary free flap closure signifies closure with a free flap later than 1 week after the trauma. In general, reconstruction of soft tissue and temporary bone stabilization may be achieved. However, definite reconstruction of longitudinal structures and bone defects is performed later (Figs. 5 and 6).

Surgical technique
Radical Debridement
A key step in surgical management and one of the most powerful tools for infection control is an early and radical debridement of devitalized, and potentially contaminated, tissue. Debridement should be performed like resection of malignancy, which means through healthy tissue and always under tourniquet control. It minimizes blood loss during debridement and alleviates evaluation of traumatized tissue. Tendons and essential neurovascular structures should be debrided and preserved, provided they are intact. In case of damage or complete transsection, essential structures should be primarily repaired either through direct coaptation or via interposition of vessels, tendon, nerve, or bone grafts.29,30
Related posts:
 Plastic Surgery
Plastic Surgery
 of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
 Versus Performance in Plastic Surgery
Versus Performance in Plastic Surgery
 Stem and Regenerative Cells in Facial Rejuvenation
Stem and Regenerative Cells in Facial Rejuvenation
 in Autologous Breast Reconstruction with Pedicled Perforator Flaps
in Autologous Breast Reconstruction with Pedicled Perforator Flaps
 Advances in Burn and Reconstructive Plastic Surgery
Advances in Burn and Reconstructive Plastic Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


