Surgical Advances in Burn and Reconstructive Plastic Surgery
New and Emerging Technologies
Keywords
• Burn reconstruction • Wound healing • Scars • Epithelialization
Wound bed preparation
Wireless Microcurrent Stimulation
Although first reported more than 150 years ago, the application of electrical field therapy to facilitate wound healing has, over the past decade, experienced a resurgence of interest. Based on several newer clinical reports and the development of noninvasive and better-engineered hardware, this technology may show promise in wound healing and is currently being tested in Europe. This technology and its potential clinical application are founded on the appreciation of existent electrical currents in both intact as well as wounded skin. Skin, depending on which area of the body is tested, possesses an electrical field of between 10 mV and 60 mV. Cell membranes possess a membrane potential, a reflection of the electrical potential difference or voltage across the membrane. Cells within intact skin are negatively charged interiorly whereas the exterior of the cell, the extracellular space, is positively charged. The difference in charge arises because cell membranes possess active and passive pumps that move sodium ions out of the cell in exchange for potassium ions, which are pumped into the cell. For the skin, this results in the epidermis being negatively charged relative to the deeper tissues, which carry a positive charge.1 When wounded and the epidermal barriers are disrupted, the skin battery is short-circuited and an outward current of approximately 30 μA/cm2 is generated and can be measured at the wound edge. Since the early 1990s, many reports have described this effect at both the tissue aand cellular levels and applications for wound healing have been proposed.2–5
Electrical currents stimulate several cell activities (eg, DNA synthesis, cell proliferation, cell migration, synthesis of the extracellular matrix, collagen, expression of growth factors, and receptors) depending on the cell type.5,6 When wounding occurs, a weak negatively charged electric field establishes between the skin and underlying tissues, termed the current of injury. It is thought that this current persists until the skin defect is repaired and that the healing process is interrupted if the current ceases. Desiccated wounds and wounds that are exposed to air exhibit a reduced electrical potential. Electrical stimulation mimics the current of injury, in effect restarting or accelerating re-epithelialization and the wound healing process.7
Electrical stimulation in wound healing is defined as the use of an electrical current to transfer energy to a wound. Studies of stimulation current effects on wound healing using a porcine model identified direct current stimulation as most effective in wound area reduction.2 Until recently, potential clinical application of these currents required using invasive transcutaneous methods of transferring current through wet electrolytic contact with the external skin surface and the wound bed, 2 electrodes having been required to complete the electric circuit.2
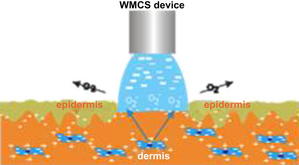
A newer method is available that uses the current-carrying capacity of charged gas molecules, oxygen and nitrogen, to donate electrons to the wound field (Fig. 1). This method is known as wireless microcurrent stimulation (WMCS). In so doing, a charge can be transferred to the wound via the air without having to touch or pierce either the wound or surrounding skin, resulting in the current of injury measurable by an amp meter. If a weak direct current electric field is applied to the atmosphere, the naturally produced N2+ and O2− move, the former in the direction of the field and the latter in the opposite direction. If the field strength exceeds a certain value, which at atmospheric pressure is approximately 3 × 106 V m−1 (3 MV/m, the breakdown field strength), a few free electrons can be accelerated to high velocities and energies, so that they can knock electrons from the oxygen and nitrogen molecules, creating more positive and negative molecules. If an O2− molecule lands on a conductive surface (like the skin), it gives up its negative charge, ceases to exist as an O2− molecule, and turns into an oxygen molecule and a few water molecules, a process termed plate-out. In this process the plated-out O2− induces a current in the wound cells and fluids whereas O2− never enters the body. In so doing, this novel approach creates a current of injury via a noninvasive electrical field that can potentially cover the total surface area of the wound (see Fig. 1).
In the authors’ burn center in Germany, WMCS is currently applied in an effort to accelerate the healing of burns wounds. A 1.5-μA current is applied as the present therapeutic basis, and all treatments are performed in sessions of 60 minutes/day per target area (Fig. 2). The return path is connected by either a wrist or ankle strap. Preliminarily the authors have found this modality easy to apply and the noninvasive, noncontact mode of application likely minimizes the risk of bacterial contamination and local trauma. Early results with this technology seem to show measurable improvement in the rate of early re-epithelialization in partial-thickness injuries; further study is under way.

Extracorporeal Shock Waves for Burn Wound Healing
Over the past several years there has been an increasing body of literature addressing the use of extracorporeal shock waves (ESWs) for healing of a variety of wound types, cellulite, and Dupuytren contracture. Several of these articles describe its use in a subset of burn wounds. In a recent article, the University of Barcelona burn unit prospectively examined its use in the treatment of 15 patients who suffered burn wounds deemed at least deep partial thickness in depth as determined by laser Doppler assessment. Wounds were treated in the emergency department on day 3 and again on day 5 postinjury. Although 1 patient was lost to follow-up and 2 patients required skin grafting, the rest healed well without surgery. Low pain scores were noted during treatment and there was a 5% incidence of hypertrophic scarring.8 Ottomann and colleagues9 investigated the effect of ESWs on wound healing in partial-thickness wounds and donor sites. In a prospective randomized trial, a group from Berlin compared time to heal after SWT with 100 impulses/cm2 at 0.1 mJ/mm2 to donor sites. The investigators noticed a significantly faster (2 days) healing. In a phase II trial with 50 patients with partial-thickness wounds a similar effect with significantly accelerated wound healing was noticed.10 The investigators concluded that a larger phase III trial is warranted.
ESW therapy (ESWT) is based on acoustic wave energy source. The exact mechanism of action of ESWT is at present ill defined.11 Many hypotheses with regard to mechanisms of action have been reported, ranging from its modulation of free oxygen radical, to decreasing apoptotic rates, and to increasing the expression of heat shock proteins as well as promotion of various growth factors, including transforming growth factor (TGF)-β1 and insulinlike growth factor 1. The latter two effects, the promotion of transforming growth factor (TGF)-β1 and insulin like growth factor 1 perhaps explain the low incidence of problem scar formation noted.12,13 Experimentally ESWT has been shown to stimulate angiogenesis and increase perfusion to ischemic tissues by increasing vascular endothelial growth factor14 while diminishing early proinflammatory immune response to deep burn injury in mice.15 Although promising, this form of therapy is in its infancy. Shock wave therapy is currently being evaluated by the Food and Drug Administration and is in phase III trials for diabetic foot ulcers.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


