Gaudet and Morestin [3] performed a transverse closure of a large umbilical hernia with resection of excess skin and fat with preservation of the umbilicus. In order to improve the abdominal contour, Weinhold [4] made a cloverleaf incision that is a combination of vertical and oblique incisions (Fig. 1.2). Desjardin [5] reported the excision of excess skin and fat weighing over 22.4 kg through an elliptical vertical abdominal incision. Morestin [6] reported five cases of massive abdominal lipectomy through an elliptical transverse incision similar to that reported by Kelly, while Jolly [7] described a low transverse elliptical abdominal lipectomy.
Babcock [8] reported using a vertical elliptical resection similar to Weinhold’s but with wide undermining of the abdominal wall (Fig. 1.3). He also dealt with the abdominal wall laxity by using a buried silver chain technique. Beck [9] makes an elliptical excision of the abdominal wall by means of two curved transverse incisions, one above the umbilicus and one below the umbilicus, leaving the umbilicus if it is not involved with an umbilical hernia. Schepelmann [10] modified the Babcock elliptical incision into a transverse teardrop incision extending from the xiphoid to the pubis (Fig. 1.4). This allowed for more contouring of the lower abdominal excess.
Frist [11] repositioned the umbilicus above the transverse incision by tunneling as in an abdominoplasty. Thorek’s [12] adipectomy was a technique of placing the incision below the umbilicus in a transverse fashion and removing the excess skin and fat down to the fascia in a wedge-shaped form (Fig. 1.5). If required, he removed of the umbilicus with a crescent excision and transplanted it to its new place at the end of the case as a composite graft.
In 1931, Flesch-Thebesius and Wheisheimer [13] modified the Thorek incision and included the umbilicus. In 1939, Thorek [14] again described his technique of plastic adipectomy. Somalo [15] used a circular anterior-posterior incision to fully reshape the abdomen. In 1949, Pick [16] reported his technique, followed by Barsky in 1950 [17], which was a modification of the Thorek transverse incision with the addition of the vertical incision at the ends (Fig. 1.6). A technique of resection in four quadrants was described by Galtier [18] (Fig. 1.7). Vernon in 1957 [19] reported his technique of low transverse incision with wide undermining and transposition of the umbilicus (Fig. 1.8). This was followed by Dufourmentel and Mouly in 1959 [20], who included the Vernon technique with the addition of a small vertical incision at the center (Fig. 1.9).
Gonzalez-Ulloa in 1960 [21] and Vilain and Dubouset in 1964 [22] reported circular abdominoplasty similar to that of Pick and Barsky (Fig. 1.6). In 1965, Spadafora [23] reported a similar technique to Vernon’s, but he lowered the incision to a less conspicuous site. His incision started at the center, curving around the mons pubis, and at the groin crease the incision curved upward toward the anterior superior iliac spine. In 1967, Callia [24] showed the use of a similar incision to Spadafora’s except the incision was placed below the inguinal crease (Fig. 1.10). Staying below the inguinal crease not only had a less conspicuous scar but also had the added advantage of some degree of lateral thigh lift.
There were three main categories of abdominoplasty up to 1967:
1.
The transverse incision
2.
The vertical incision
3.
A combination of vertical and transverse incisions (Fig. 1.11)
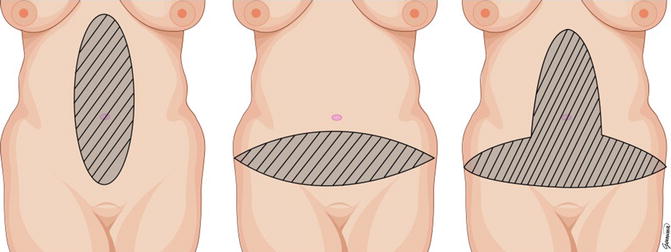
Fig. 1.11
(Left) transverse incision; (middle) vertical incision; (right) combined incisions
After 1967, there were many modifications of Callia’s technique, but surgeons started favoring the low transverse, inconspicuous scarring.
In 1967, Pitanguy [25] published his technique that was considered to produce successful results. From 1967 to 1975, he reported more than 500 cases of abdominoplasty and mammaplasty at the same time [26]. Pitanguy not only favored a low transverse abdominal and groin incision but also advocated extensive undermining over the costal margins, muscle tightening, and compression dressing (Fig. 1.12).
The “W” technique incision by Regnault [27] appeared in 1972. This was later modified in 1975 [28
 Abdominoplasty Combined with Cesarean Section: Discussion of the Evidence
Retrospective Analysis of Never Events in Panniculectomy and Abdominoplasty Patients and Their Financial Implications
Abdominoplasty Combined with Cesarean Section: Discussion of the Evidence
Retrospective Analysis of Never Events in Panniculectomy and Abdominoplasty Patients and Their Financial Implications
 No Drain Abdominoplasty with Progressive Tension Suture: The Logic, Simplicity, and Aesthetics
No Drain Abdominoplasty with Progressive Tension Suture: The Logic, Simplicity, and Aesthetics
 Evolution of the High-Superior-Tension Lipoabdominoplasty: The High-Tension Abdominoplasty
Evolution of the High-Superior-Tension Lipoabdominoplasty: The High-Tension Abdominoplasty
 Circumferential Abdominoplasty
Circumferential Abdominoplasty
 Abdominal Wall Repair Post Hernia in Kidney and Liver Transplantation
Abdominal Wall Repair Post Hernia in Kidney and Liver Transplantation




Related posts:
Abdominoplasty Combined with Cesarean Section: Discussion of the Evidence
Retrospective Analysis of Never Events in Panniculectomy and Abdominoplasty Patients and Their Financial Implications
No Drain Abdominoplasty with Progressive Tension Suture: The Logic, Simplicity, and Aesthetics
Evolution of the High-Superior-Tension Lipoabdominoplasty: The High-Tension Abdominoplasty
Circumferential Abdominoplasty
Abdominal Wall Repair Post Hernia in Kidney and Liver Transplantation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
