Fat transfer has become the primary method for facial rejuvenation in my clinical practice for all ethnicities. This technique can be effectively used to address panfacial volume loss so long as artistry, technical skill, and an in-depth understanding of fat grafting changes over the years are well applied and understood. Fat grafting can replace many traditional facial rejuvenation techniques or serve as an important adjunct to excisional and lifting procedures to temper the degree of excision and lifting that are required.
Commonalities and differences exist for managing the aging face of the ethnic and nonethnic individual. This article explores the intersection and divergence of strategies for facial rejuvenation through the filter of a new paradigm for the aging face. This new paradigm is, in effect, the opposite of traditional lifting- and excisional-based rejuvenative surgery. Using facial fat transfer, adding to the face rather than subtracting from it, defines the new paradigm. Although facial fat transfer is universally applicable to almost any individual who undergoes aging, it is particularly beneficial for the ethnic face as a standalone procedure on many counts. First, many ethnic individuals of varying origins have greater skin melanin content that serves as a protective barrier against solar aging, which can create cutaneous elastosis and dyschromias. Accordingly, the aging process, particularly in dark-skinned individuals, can be almost entirely a manifestation of volume depletion with little evidence of gravity and skin damage. In addition, fat transfer can be used as a sculpting method to soften ethnic features and facial shape to create a more balanced appearance. This topic is studied in more depth in this article. Facial fat transfer can be a potent and primary method for reversal of aging in ethnic and nonethnic populations.
Before the role of facial fat transfer in different ethnicities can be understood, the logic behind its use in all individuals must be considered. Adding more adipose to an eyebag, fat to an already ptotic brow, or fat to a seemingly heavy jawline seems counterintuitive. Accordingly, how facial fat transfer is perhaps a revolution in thinking and approach to the aging face (in short a new paradigm) must be defined at the outset. The best way to regard facial fat transfer is to begin with the educational process of understanding and perceiving negative space. For example, rather than seeing the steatoblepharon of an eyebag, the eyebag can be considered to represent the fat that remains after a great percentage of fat has dissipated along the orbital rim and midface. Similarly, instead of seeing drapage of upper-eyelid skin and a ptotic brow, it can be envisaged that the bony orbital rim becomes more exposed over time and that the convexity of the brow contour needs to be restored rather than elevated due to perceived gravity (which in reality plays a negligible role in the brow). The best way to understand this phenomenon of deflation rather than gravity is to start with the patient’s old photograph, which in almost every case exemplifies a fuller brow contour rather than an elevated one. The brow is one of the most difficult areas to understand that deflation rather than gravity is at play. The reader is encouraged to think of the brow as a balloon that deflates over time creating the perceived effect of sagging; filling would give the best results.
Currently, I rarely perform a browlift, because I find that it is simply unnecessary and, in many cases, counterproductive. The longer, almond-shaped eye of youth gives way to a bonier, rounder look that is exacerbated by browlifting and aggressive traditional blepharoplasty. In almost every circumstance, periorbital fat transfer is the mainstay of rejuvenative intervention that I rely on, and, in conjunction, I occasionally perform traditional blepharoplasty to enhance my fat transfer result rather than as a substitute for it. I perform an upper-eyelid blepharoplasty with a fat transfer for the upper-eyelid/brow complex only when it is warranted, which is in approximately 1 in 5 patients. I prefer a selective skin-only blepharoplasty, removing 2 to 3 mm of redundant skin, in the following cases:
- 1)
When the eyelid skin hangs at or below the ciliary margin
- 2)
When the skin edge appears “crêpey” and irregular, or preferably an upper eyelid that manifests both of these conditions
The reason to remove the extra skin in the case of skin irregularity is apparent. The reason to remove skin when the skin hangs at or below the ciliary margin is to minimize the drooping eyelid look if some of the fat resorbs and fails to achieve the desired esthetic objective.
With lower-eyelid steatoblepharon, the need to remove fat from the perceived eyebag is rarely indicated and the need to remove redundant skin almost never arises. I prefer to perform fat grafting alone for the lower eyelid in almost every case but, in approximately 1 in 10 cases, I perform a concurrent transconjunctival lower-eyelid blepharoplasty to manage the extra fat that will not, most likely, be sufficiently camouflaged with fat grafting to the inferior orbital rim. The situation in which I prefer a transconjunctival blepharoplasty with fat grafting to the inferior orbital rim involves eyebags that are so protuberant that they extend well beyond the orbital rim in an anterior-posterior position. In fastidious individuals who want the absolute best results for the lower eyelid, I offer to perform a concurrent lower-eyelid blepharoplasty but still try to manage expectations that there might nevertheless be some remaining perceived steatoblepharon. I almost never remove extra skin from the lower eyelid but instead choose to manage rhytids and flaccidity of the lower eyelid with skin resurfacing and botulinum toxin therapy. I find that traditional skin-muscle flap blepharoplasty carries too high a risk of changing the shape of the eye by altering the lateral canthus even slightly in any direction (medially, laterally, inferiorly, or superiorly).
Many patients (and surgeons) are surprised at how much the midface affects the look of the eyes. The gaunt, flattened terrain of the aged midface can contribute more significantly than almost any other facial feature, including the eyelids themselves, to the tired appearance of an eye. To help patients (and surgeons) appreciate the effect that a fuller midface contour has on the look of the eyes, I gently nudge the cheek into a fuller, rounder contour by pushing it up from below with my thumb to simulate volume (not lifting) and have the patient see that, with this maneuver, even though the lower-eyelid contour may be worsened, the eyes look more alert and the face looks markedly more rested in appearance. To understand why a malar implant fails to rejuvenate the midface, one must understand how an aged midface ages. With volume loss to the midface as people age, the bony malar eminence becomes more exposed (ie, the bony prominence is the hallmark of aging). A solid implant on the malar eminence worsens this bony look and thereby exacerbates aging. Fat transfer covers the bony prominence and blends it in with the surrounding contour depressions. Similarly, midface lifts fail to work because they lift deflated tissue upward and stretch the skin more over exposed bony terrain, which ultimately does not resolve the core issue, that is, volume depletion of the midface.
I mentally divide the central cheek into 3 zones (minus the buccal area, to be discussed later). The central anterior cheek, which corresponds with maximal cheek deflation along the mediosuperior to inferiolateral line of the malar ligament, is perhaps the most important region to fill for aging in most individuals. Pushing this area too forcefully can create an overexuberant appearance to the cheek and also over feminize a masculine face. The lateral cheek is defined as the region that overlies the malar bony eminence. In gaunt narrow faces, I prefer to augment this region more aggressively than in heavier faces or in individuals with prominent cheekbones. Trying to balance a face is an underlying objective with any facial esthetic endeavor (ie, creating harmony between various sizes of neighboring facial structures, without greatly disturbing personal identity). The lateral cheek also serves as an important area to augment for men to create a more structured outer cheek shape that can be masculinizing. The lower, medial, anterior cheek, which rests directly above the nasolabial groove and partially defines the upper border of the nasolabial fold, should almost never be augmented. It tends to become more pronounced in heavier individuals and makes the cheek look ptotic and heavy. Accordingly, in more heavily set individuals, placing fat more superiorly and centrally can offset this heavy appearance and create a relative narrowing of the face. Modest amounts of fat should be used in order not to create too fat a face.
The buccal area can be one of the most important areas to fill or one of the most important areas to avoid. In the heavier patient, the buccal region appears full and heavy. Filling the central upper anterior cheek as mentioned can make the buccal area appear smaller in these individuals. However, in the gaunt face, the buccal area can be a central focus to enhance to make the face appear more youthful. Most often, traditional perspectives for the aging face concentrate on the upper, mid, and lower faces; however, I look at the buccal area as an important transition point between the middle and lower faces. Unifying the face that becomes more markedly disjointed and separate with aging is an important goal in facial rejuvenation, and filling the buccal area facilitates this goal by unifying the stark transition between an augmented cheek and an augmented and lifted lower face. Mentally, I have divided the buccal region into 3 zones: the medial buccal hollow, the central buccal hollow, and the lateral (subzygomatic) buccal hollow (which I also refer to more colloquially as the backfill zone).
The central buccal hollow is self-evident and corresponds to the most obvious central buccal depression, which can be a focal point of interest for filling. In more aged individuals who have lost dentition, I conceptualize a more medial extension of the buccal hollow that corresponds with the upper arch of teeth/maxilla. If this area is filled, the labiomandibular groove (marionette) line can be temporarily exacerbated for several weeks, or with aggressive augmentation can be permanently worsened. The patient should be aware of this possibility. In my opinion, fat grafting is not a reliable option to fill linear fold defects like the nasolabial groove or the labiomandibular groove. Other options must be used to manage the fold with more consistent outcomes. The gaunt patient is particularly helped by filling the lateral buccal hollow, which corresponds with the region that falls immediately inferior to the zygomatic arch/bony malar eminence. Patients who have had a standard SMAS-ectomy rhytidectomy and who have lost volume to the outer face and are already predisposed toward being gaunt are greatly assisted by filling this lateral backfill region. In any circumstance, after augmenting the midface/cheek region, the surgeon may create a relative buccal hollow that should be addressed at that point to soften this accentuated transition. Women do not aspire to looking fat, so buccal augmentation must be undertaken after meticulous and detailed consent and discussion with a patient.
The chin/anterior jawline is another important area to augment in the aged face. A lower face and neck lift can manage the jowl and the neck but the patient may still not appear as refreshed as possible. A chin implant is also not necessarily the answer, as can be understood through the concept of the inverted U. Most surgeons and patients are focused on the jowl and the labiomandibular groove as the problem areas; however, a new concept that I have developed focuses on the inverted U shape of bony exposure that occurs with aging. The upper anterior chin that lies just medial to the labiomandibular groove should be the focus of attention, as this depression creates the starkest relief of aging but is also the least understood or managed. The lower limb of the inverted U corresponds to a region known as the prejowl depression; that is, the recess of soft tissue immediately in front of the jowl itself.
As mentioned earlier in this article, to understand these concepts the surgeon must begin to see negative space well. Seeing positive space problems such as the jowl and the fold addresses only part of the problem with aging. Seeing negative space (hollowness, bone exposure) is integral to a successful vision and the design of a treatment protocol. An extended chin implant helps to address the lower limb (prejowl) of the inverted U but worsens the upper limb of the U, which can be one of the most important areas to work on. Fat grafting to the jawline can eliminate the need for a lower facelift or significantly improve a facelift result.
An area that I address less commonly is the lateral mandible; however, it can be an important area to fill in select individuals. For instance, the most common indication that I have to address the lateral mandible is found in the older patient who has in the past undergone a lower SMAS-ectomy rhytidectomy that has caused further worsening of volume loss across the lateral mandible, where the bony prominence of the mandible is completely exposed leading to more aging. When the buccal area is filled in these individuals, the picture still seems incomplete, given the extended lower lateral loss in the mandible. Filling the lateral mandible can support the buccal fill by creating a more unified extension of the buccal fill. A second indication is loss of bone in the lateral mandible, which is typically present following previous orthognathic mandibular advancement. The patient can look cheek-heavy, which would only be worsened with anterior cheek filling, without support to the lower lateral face. The concept of facial balance is reiterated here. Finally, a prominent jowl in an individual who refuses to undergo a proper rhytidectomy can be better effaced by filling in front of (prejowl) and behind (postjowl) the jowl itself. The only caution is that many individuals who exhibit a prominent jowl may also be slightly more heavily set in the jowl and mandate a more targeted approach to the immediate postjowl defect without significant lateral extension so as not to widen the face and render it heavier in appearance.
There are some important major limitations of fat transfer. First, fat grafting is principally intended to manage soft-tissue loss of the face and not necessarily bony weaknesses. For more predictable projection of the mandible, an alloplastic chin implant is still mandated with or without fat grafting. The cheek region can almost always be better managed in aging simply with fat grafting, as minor bony weaknesses can be camouflaged with soft-tissue augmentation with fat transfer. Similarly, minor degrees of chin retrusion can also be camouflaged with fat grafting. However, excessive fat transfer to the chin to address what a chin implant would otherwise have done better, will most likely create a fat-appearing chin, which is obviously unesthetic. Second, fat transfer is not indicated to manage lip augmentation, which causes unduly protracted edema/distortion and is associated with a high resorption rate. As mentioned earlier, grafted fat also has too soft a consistency to consistently lift away the labiomandibular and nasolabial groove depressions.
I have likened fat grafting to hair grafting, because of their similar nature, trajectory, and outcomes, to help individuals better understand fat grafting using the model of hair transplantation. Fat grafting and hair transplantation use a tiny micrograft that is suspended in a network of surrounding native tissue that requires ingrowth of blood supply to mature and grow over time. Accordingly, fat grafting results (if done properly with surviving grafts) look best approximately 2 years following fat transfer when the graft is fully vascularized. Using the model of hair restoration, a transplanted hair graft survives for the first few days via plasmatic imbibition. Over the following few months, the graft continues to survive using a process of primary then secondary inosculation. Only after 6 months is the graft formally supplied via neovascularization. At that point, the hair graft grows and improves and continues to do so for approximately 18 months. Fat grafting looks good for the first month to 6 weeks because of edema that mimics a fat-grafting result. However, at 3 months, when all swelling has dissipated and the fat graft has not fully established its blood supply, it may not look so good. Starting at approximately 6 months, the fat-grafting result begins to improve steadily for approximately another 12 to 18 months just as a hair transplant result does (obviously only if the surgeon can assure graft survival). Because fat is not a bioinert substance like injectable hyaluronic acid, it must be respected as a live graft. Weight changes can influence the result, so obese individuals or those with poorly controlled weight, are not necessarily good candidates. Using fat to fill small surface defects, like acne scars, is unadvisable because the live graft may create bumps and lumps as the fat grows asymmetrically in these areas. Similarly, using fat to fill asymmetric facial defects is potentially fraught with problems if the fat graft gains robust blood supply or if the patient’s weight fluctuates. It is as important to understand these limitations as it is to understand the esthetic benefits of fat transfer.
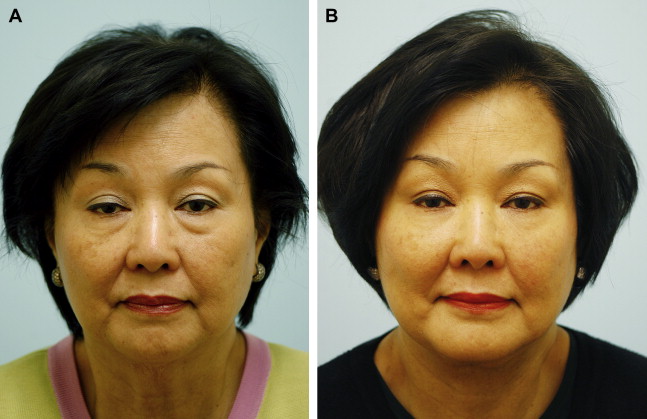
With this foundation of understanding, the different way in which fat transfer can be applied to the ethnic face compared with the nonethnic face can be understood. The term ethnic encompasses a broad demography including Asian, African, Hispanic, and Middle Eastern. However, some universal concepts may be applicable. In certain ethnicities, such as Asian and related ethnicities, a wider facies may be the norm. In these cases, fat grafting may be considered a less-than-ideal treatment option. On the contrary, fat grafting can be used to accentuate the chin and anterior cheek to effectively narrow the facial shape ( Fig. 1 ). In addition, in more melanin-protected races, volume depletion can be the principal, or only, manifestation of significant aging. By addressing this element of aging, most of the aging can be effectively corrected.
Related posts:
 Hair Restoration in the Ethnic Patient and Review of Hair Transplant Fundamentals
Hair Restoration in the Ethnic Patient and Review of Hair Transplant Fundamentals
 Midface Alloplastic Augmentation in the Asian and Latino Patient
Midface Alloplastic Augmentation in the Asian and Latino Patient
 Middle Eastern Rhinoplasty
Middle Eastern Rhinoplasty
 Lower Facial Rejuvenation in the Non-Caucasian Face
Laser Treatment for Ethnic Skin
Rhinoplasty in the Patient of African Descent
Lower Facial Rejuvenation in the Non-Caucasian Face
Laser Treatment for Ethnic Skin
Rhinoplasty in the Patient of African Descent
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


