Fig. 1
Clinical picture of the bone defect

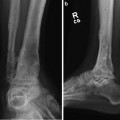
Fig. 2
Three-dimensional CT reconstruction of the leg. Contrast agent was utilized for detecting a vascular injury
3 Preoperative Problem List
1.
Polytraumatized patient
2.
Left hip dislocation
3.
Type 3 open femoral fracture (subtotal amputation)
4.
Massive bone defect with absent patellar tendon
5.
Vascular injury (femoral vein laceration)
6.
Contaminated soft tissue
4 Treatment Strategy
(a)
Closed reduction of the hip dislocation.
(b)
Mounting of a joint-bridging external fixator.
(c)
Vascular repair of the femoral vein.
(d)
Fasciotomy of the upper and lower leg and temporary coverage with synthetic skin.
(e)
Custom-made spacer with bone cement and K-wires was placed into the bone gap (07/2010).
During the following weeks,
The leg length discrepancy was treated by:
In the last step,
(f)
Several revision surgeries and changing of the Vacuum assisted closure (VAC) was performed until
(g)
Split-skin graft covered the soft tissue defect (08/2010).
(h)
Mounting a monotube on the femur
(i)
A multiplanar ring fixator on the tibia. Osteotomies were performed just below the lesser trochanter and below the tibial plateau.
(j)
A Hoffman fixator was added to connect the two frames in the knee region (09/2010).
(k)
An arthrodesis nail was inserted after frame removal to reduce the consolidation time in the frame and to realign all fragments (05/2011).
5 Basic Principles
1.
Anatomic joint reconstruction in cases of severe or destroyed articular fractures is usually not possible in the initial damage control surgery. In these cases a joint-bridging external fixator is useful to protect the soft tissue, to stabilize the joint when severe ligament injury is present, or when a vascular repair has been performed.
2.
Vessel injuries commonly occur in multiple-injured patients especially in the lower extremity. Direct injuries are caused by sharp and stump violence, indirect mechanisms by tension, distraction, or torsion. The diagnosis or suspicion of a vascular injury begins with the clinical investigation. Hard signs include active hemorrhage, large expanding or pulsatile hematoma, absent palpable pulses distally, and distal ischemia.
3.
Early surgical soft tissue debridement
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
