Fig. 1
Pre-operative clinical photo demonstrating ulceration over the tophi and medial eminence

Fig. 2
Pre-operative clinical photo demonstrating hallux valgus deformity and a gouty tophi over the medial eminence

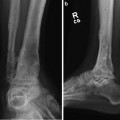
Fig. 3
Radiograph demonstrating sever hallux valgus with a medial gouty tophi
3 Preoperative Problem List
Deep infection involving soft tissue and bone
Severe deformity (metatarsus adductus primus with hallux valgus) resulting in a pressure ulcer over the medial metatarsal head
Uncontrolled gout
4 Treatment Strategy
In order to salvage the big toe, three goals must be met. First is to debride and eradicate the infection. Second is to correct the underlying deformity to prevent pressure over the medial first metatarsal head. Third is to control the gout.
Debridement should include excision of the gouty tophi and all nonviable soft tissue and bone. A wedge resection of the skin and tophi was planned to adequately debride the gouty tophi and overlying redundant and nonviable skin.
Once debridement has been accomplished, then alignment should be addressed. One could perform a proximal osteotomy to correct the metatarsus adductus primus. However, in this case, performing an osteotomy in an already infected case runs a high risk of complication including nonunion of the osteotomy and/or wound infection. Therefore, a fusion at the metatarsophalangeal joint (MTP joint) with partial correction of the deformity is preferred as simpler solution. One only has to perform enough correction to prevent future ulceration.
For fusion, one could utilize internal fixation; however, with the active infection and potential for wound breakdown, external fixation is more optimal in order to keep foreign material out of the infected zone.
5 Basic Principles
Keeping hardware away from infected bone helps to eradicate the infection. In this case a mini-rail external fixator was chosen, and culture-specific antibiotics were administered for 6 weeks post-op. This external fixator has a universal joint that is placed over the center of rotation for the first metatarsophalangeal joint. The fixator also allows for excellent compression at the time of surgery and then continued adjustable compression in the weeks post-operatively. It also allows for stable fixation and access to complicated wounds for ongoing wound care. All of the principals combine to result in a successful outcome and salvage of the big toe.
6 Images During Treatment
See Figs. 4, 5, 6, 7, 8, 9, and 10
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
