Fig. 1
Pre-operative anteroposterior-view radiograph of the right foot obtained at initial presentation. Note the loss in joint space and hallux rigidus

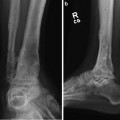
Fig. 2
Pre-operative lateral-view radiograph of the right foot obtained at initial presentation. Note the periarticular osteophytes and the elevation of the first metatarsal
3 Preoperative Problem List
1.
First metatarsal phalangeal joint arthritis (Hallux Rigidus)
2.
First metatarsal phalangeal joint osteophytes
3.
First metatarsal elevation
4 Treatment Strategy
Indications for first MTPJ distraction are congruent joint surfaces, pain, joint mobility, and moderate to severe arthritis (Regnauld stage II or II). The indications may be stretched to include avascular necrosis of the first metatarsal head. Joint distraction reduces the mechanical stress on the cartilage by using an external fixation device and provides an interval healing of the cartilage surfaces.
Realignment of the soft tissue and bone is as critical to joint preservation as the joint distraction technique to obtain maximum benefits. Therefore, I utilize adjunctive procedures combined with hinged joint distraction to maximize great toe joint preservation which includes cheilectomy, osseous realignment of the metatarsal/phalanx, soft-tissue rebalancing, and resection of osteophytes/loose bodies as required. Procedures such as core decompression, micro-fracture of osteochondral lesions, intra-articular injection of human growth hormone, and digital nerve decompression are also utilized when necessary.
5 Basic Principles
Joint distraction (ligamentotaxis) with external fixation for a 2-month period reduces joint loading and provides an environment in which the joint cartilage can recover. Studies have confirmed that fibrocartilage forms to restore the arthritic joint surface during distraction treatment (Salter et al. 1980; Lafeber et al. 2006; Hung et al. 1997). Joint distraction also produces a decreased thickness of the subchondral bone, which is beneficial to increase the resiliency of the entire joint cartilage and fibrocartilage overlying the subchondral bone. Hinged joint distraction with external fixation allows range-of-motion exercises and weight bearing (intermittent hydrostatic joint loading) during treatment, which increases the synovial fluid and thus provides healing of the joint cartilage.
The goals of the first metatarsal phalangeal joint distraction with external fixation are to decrease pain and improve function. Joint pain is diminished by the formation of fibrocartilage, which adequately seals the cartilaginous cavity to the subchondral bone cyst and therefore eliminates increased fluid pressure and pain (Abraham et al. 2012). The formation of fibrocartilage is the reason why joint distraction leads to lasting pain relief of osteoarthritis of the ankle joint. Joint distraction typically will not improve the amount of joint range of motion but more importantly can alter the arc of motion. I employed the approach of performing blocking osteophyte resection, muscle and joint contracture release, and osseous realignment procedures along with hinged joint distraction which has been clinically successful.
6 Images During Treatment
See Figs. 3, 4, 5, 6, and 7.

Fig. 3
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
