8 Adjunctive Methods in Cleft Palate Repair and Complications
Introduction
Cleft palate repair was first described in the early 1800s, and today several techniques exist that have been well described and successfully employed. The methods for cleft palate repair are well established and, regardless of the procedure used, experienced surgeons typically have excellent outcomes using these traditional methods. Despite this, all surgeons are occasionally faced with particularly challenging repairs or complications of cleft palate surgery. Appropriate use of adjunctive techniques during a difficult closure is a critical component of any cleft surgeon′s armamentarium and can help minimize the chance of complications. Complications, once they occur, can be incredibly challenging to treat and require the surgeon to be able to call upon several possible treatment options. This chapter reviews adjunctive techniques for use during cleft palate surgery as well as management of common complications.
Primary Cleft Palate Repair
Complications
The goals of primary palate repair are to close the cleft in its entirety and to restore the palatal anatomy into a more anatomic state, thereby improving both feeding and speech. While the functional principles of palatoplasty are to restore the palatal muscular sling and re-create a separation between the oral and nasal cavities, the surgical principles include multiple layer closure, atraumatic technique, and a tension-free closure. These tenets of surgical technique can be difficult to uphold in the setting of wide and/or difficult clefts. In the scenario of an extremely wide cleft palate (> 20 mm), the surgeon may be faced with undesirable tension on the closure or inability to completely close the cleft. If not appropriately managed, this might then lead to secondary complications—the most dreaded being palatal flap death from vascular compromise. A feared intraoperative complication, but rarely encountered, is avulsion of the greater palatine vascular pedicle. Postoperative complications can include hemorrhage, infection, wound dehiscence, and oronasal fistula. Fistula formation after primary repair most commonly occurs at the junction of the hard and soft palate, which is where there is no muscular layer in the repair.1 A multitude of factors may play a role in failure of the cleft repair, but the severity of the cleft size is related to fistula formation postoperatively. Musgrave and Bremner in 1960 reported an association of fistula rates with increasing cleft width: 4.6% for incomplete cleft palate, 7.7% for complete unilateral cleft palate, and 12.5% for complete bilateral cleft palate.2 Further, other confounding factors can contribute to this complication including increased closure site tension, postoperative infection or bleeding, trauma, and poor surgical technique.3,4 One report from East Asia even showed increased fistula rates in association with a severe acute respiratory syndrome outbreak in Hong Kong, but was unable to definitively establish cause–effect relationship in this bizarre finding.5 The issue raised by these studies, however, highlights that optimal conditions are absolutely required to minimize the rate of fistula formation.
Techniques
Some of the factors that complicate cleft palate repair are beyond the control of the surgeon, but reducing poor outcomes calls for strategies to minimize these factors. Of the numerous techniques described for primary cleft palate repair, each surgeon must match the technique with which they achieve the best outcomes, while taking into account the slowly emerging evidence base that supports specific algorithms (see Chapter 7).
Improving outcomes with the particularly wide cleft may include the use of simple surgical maneuvers such as the use of lateral palatal relaxing incisions or management of the tensor veli palatini and hamulus. Others have reported mobilization of the nasal mucosa beyond the typical dissection, utilizing tissue posterior to the eustachian tube orifice.6 These relatively quick and simple techniques can all contribute to reduced tension, but are supported by low-level evidence (sparse prospectively comparative study).
Several extensions of the typical palate repair, which seem to improve outcomes, have been reported in the literature. The greater palatine artery pedicle can be carefully skeletonized to increase mobility of the palatal flap prior to closure.7 This method is relatively safe, simple, and similar to the greater palatine artery island flap used for reconstructing soft palate defects in oropharyngeal cancer. Careful dissection of the neurovascular pedicle has been described with a nerve hook.8 Proper identification of the arterial pedicle is critical during dissection to avoid inadvertent injury to the vessel. There are fibrous attachments that run along the pedicle and into the foramen. Careful dissection of this tissue greatly improves mobilization of the pedicle and the corresponding ipsilateral hard palate flap.
More rarely, the greater palatine foramen can be carefully fractured with an osteotome, releasing the vascular pedicle for greater length and reach.8 Consideration can be given to performing a careful osteotomy on the foramen if aggressive pedicle dissection does not result in adequate flap mobility. Some advocate the use of incisions through the periosteum on either side of the pedicle as it runs along the hard palate. This maneuver reduces the amount of periosteal attachment along the pedicle to further improve the mobility of the flap. In one study, this technique of reducing tension on the wound closure resulted in reducing fistula rates from 10.6% to 2.1%.7
Recently, the use of cadaveric acellular dermal matrix has become a popular adjunct to cleft palate closure in the particularly difficult primary palatoplasty. This material may be incorporated during the closure of the oral and nasal lining as an added barrier against fistula formation and is typically placed overlying the posterior hard palate and the muscular layer of the anterior soft palate. Using a thin sheet of matrix promotes ingrowth of native tissues and reduces the risk of extrusion (see Fig. 7.13). One report suggests that a small 1- to 2-mm gap in the oral mucosa only may be left if excess tension exists.9 It is hypothesized that the material acts as a physical barrier, a bridge for epithelial migration, and may even increase the tensile strength of the wound secondary to fibrosis. Ingrowth of epithelial cells occurs secondary to basement membrane proteins (such as laminin and type IV collagen) that act as adhesion molecules.9 The matrix serves as a lattice on and through which the epithelial cells can move. When compared to skin grafts, cadaveric acellular skin matrix is associated with less scar contracture. This is a particularly important issue in palatoplasty, where the final length of the palate is a critical variable in preventing further surgery and ultimately improving the final functional outcome.
The decision to use an interpositional graft (allogenic or autologous) in palate closure and indications for its use are not entirely clear from the current level III evidence. Clark et al.9 recommend the addition of this matrix for palates > 15 mm, but another small study has shown improved fistula rates (3.2% compared to the reported 10 to 23%) in a series of consecutive Furlow palatoplasties performed on cleft widths ranging from 8 to 15 mm.1,9
Secondary Palate Repair
Patients who have failed primary palatoplasty with subsequent fistula formation pose a complicated and difficult treatment scenario. At baseline, fistula repair is more difficult than primary repair due to the intrinsic changes in scar tissue, which include compromised vascularity, excessive scarring, fibrosis, and subsequent limitations in the range of motion in the palatal tissue.3 Multiple procedures have been described for treatment of the postoperative fistula, and each surgeon must tailor these various techniques according to the individual characteristics of each fistula. The key component for any fistula repair is a two-layered water-tight closure. This creation of two layers poses the opportunity for augmentation of each layer by various reconstructive methods (nasal lining and oral lining) and the creation of a new “middle” layer with adjunctive material. The remainder of this section focuses on the various techniques used in the closure of these three layers.
Nasal Lining
If the nasal or oral lining is deficient, then further procedures must be performed to recruit extra tissue for closure. Certainly extended nasal lining mobilization (as described for primary palatal repair above) may recruit mucosa from the nasal floor and lateral nasal wall, but in a secondary repair, this may be difficult secondary to scarring and fibrosis.
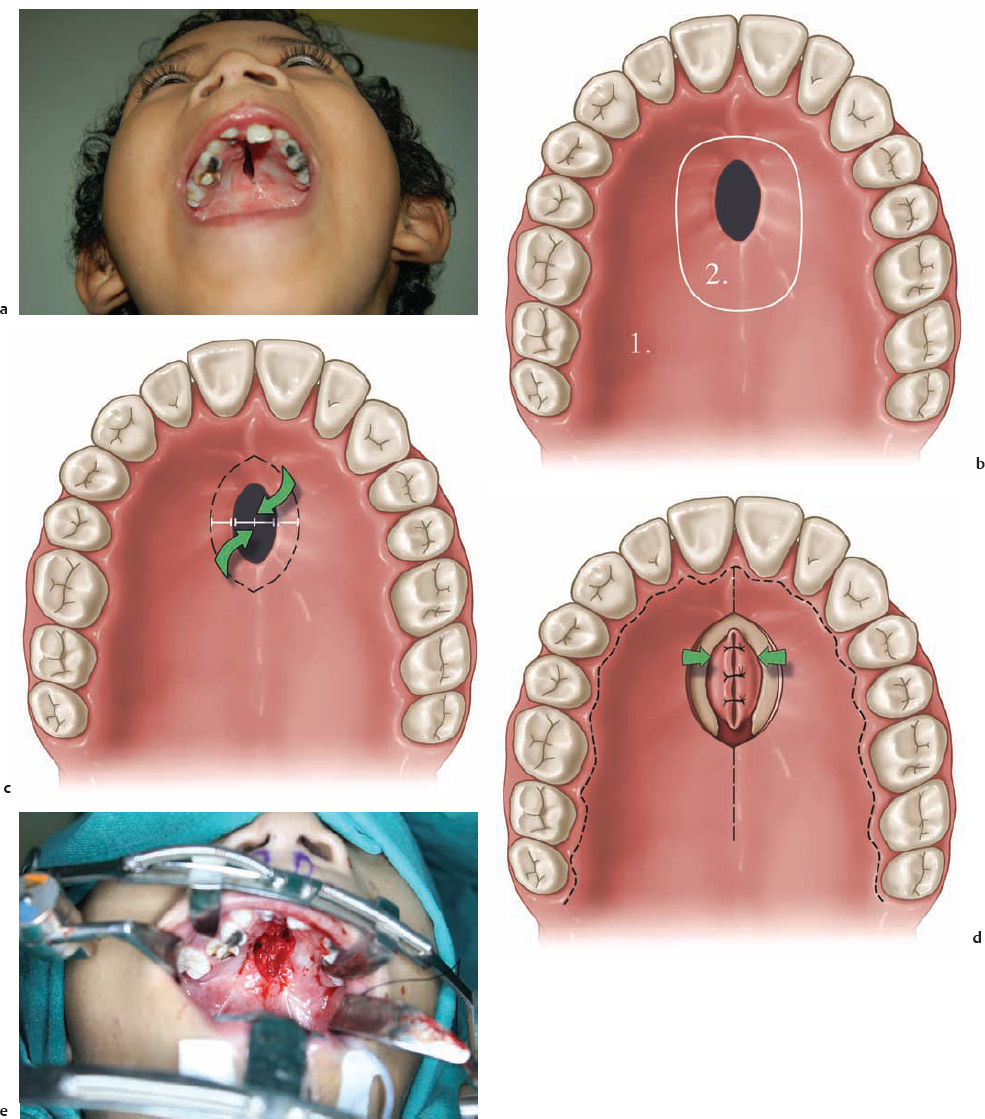
Turn-in or turn-over flaps are the most popular initial technique for the closure of the small postoperative fistula. There is no prospective data in the literature that critically evaluates this technique, but it is a traditional approach to fistula closure. This flap is based on the edge of the fistula and extends laterally to a length that is at least equivalent to the diameter of the fistula. The cuts are made through the periosteum and the flap is raised in this subperiosteal plane. The flap is then turned over so that the mucosa is facing the nasal side. The opposing side of the fistula is also incised but 1 to 2 mm away from the edge. This thin strip of mucosa is also turned inward and forms the attachment point for the lateralmost edge of the turnover flap. These edges are sutured together with absorbable suture (Vicryl [Ethicon, Somerville, NJ] or polydioxanone) and complete the closure of the nasal layer. Alternatively, the turn-in flap can be constructed by making a circumferential incision around the fistula ( Fig. 8.1a,b ). The mucosal flaps can then be turned inward and sutured together using absorbable suture to create a new nasal lining ( Fig. 8.1c,d ). Turn-in flaps do have some limitations to their use. They can only reliably be used to close small fistulae. Being immediately adjacent to a fistula, the tissue may have poor vascularity and mobility. Furthermore, the edge of the fistula is not excised using this technique but rather is incorporated into the repair, thus placing chronically scarred tissue into the nasal lining.
If additional tissue is still required, the inferior turbinate mucosal flap presents an excellent option. The flap has a hearty blood supply and the surface area of the recruited mucosa is actually quite large. Further, it may be pedicled anteriorly or posteriorly, providing flexibility in the geometry of the flap design to accommodate a number of different defects. The technical details of this flap are beyond the scope of this chapter, but this technique is certainly an important adjunct and should be considered for difficult cases.
“Middle” Lining
A “middle” lining between the nasal and oral mucosal layers (i.e., interpositional graft) may be created by the insertion of an acellular dermal matrix. An evidence-based review of this technique showed a nearly 5% increase in the closure rate (12.9% historical rate of fistula decreased to 8.1%) for a combined 74 patients (cumulative data from five studies).3 Three other small studies also utilized acellular dermal matrix and had similar results with 100% closure rates.10–12
A single retrospective study utilized mastoid fascia as a middle lining and achieved closure in 14 of 16 patients. This material may make a suitable replacement for the middle lining when acellular matrix is not available. However, this study lacked a control group and did not directly compare results to those using acellular matrix.4
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


