Fig. 1
Pre-operative lateral photograph of the equinus contracture and lack of heel purchase. Note the previous lateral incision due to open reduction and plating of the distal fibula fracture

Fig. 2
Pre-operative axial photograph of the equinus contracture. Note that an open posterior approach and Achilles tendon lengthening failed to correct the deformity. The patient presented with a complaint of pain in the ankle and inability of the heel to touch the ground

Fig. 3
Pre-operative lateral view radiograph showing fixed equinus of the ankle at 20°
3 Preoperative Problem List
Equinus contracture (fixed at 20°)
4 Treatment Strategy
Equinus contracture secondary to a post-traumatic lower extremity fracture is common when the patient is not properly immobilized in a 90° position during the healing phase of a lower extremity fracture. In this case no open tendon lengthening or joint releases where needed; only gradual distraction of the ankle to 8–10 mm with gradual ankle dorsiflexion correction of the equinus was performed. All toes where pinned to avoid digital flexion contractures during the gradual equinus correction. A prophylaxis tarsal tunnel decompression was performed at the time of application of the external fixation. The goal of correction was to dorsiflex the ankle to 10° above neutral; therefore, a total correction of 30° of dorsiflexion was performed. The rate of correction can be calculated by measuring a ratio of the distance between the center of rotation of the ankle joint (lateral process of the talus) and the posterior distraction rod compared to the Achilles tendon. Typically this is a 3:1 ratio, whereby if the posterior distraction rod is turned at a rate of 3 mm/day, the Achilles tendon is lengthening at 1 mm/day. Once the needed ankle dorsiflexion is obtained that position will be maintained for 6 more weeks until removal of external fixation and range of motion exercises can be performed by temporary removing the posterior rod.
5 Basic Principles
Gradual ankle distraction for treatment of equinus contracture does not create further scarring of the ankle joint like an open approach would. Thus gradual correction with external fixation maintains or improves the ankle joint range of motion. A prophylaxis tarsal tunnel decompression was performed and is recommended in post-traumatic ankle deformity correction. With gradual ankle contracture correction with external fixation, a prophylaxis tarsal tunnel decompression is recommended in a correction of 25° or more (Lamm et al. 2007). Pinning of the toes is recommended if a toe contracture exists prior to gradual correction. Also pinning of the toes is recommended if the amount of gradual correction is large, to avoid digital flexion contractures during correction.
6 Images During Treatment
See Figs. 4, 5, 6, and 7.
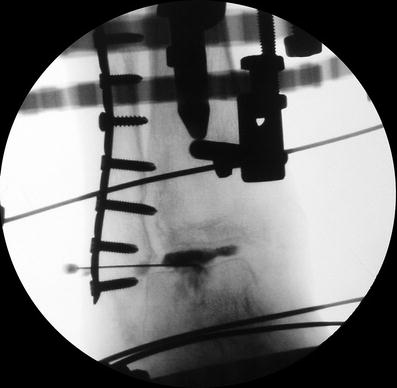
Fig. 4
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
