Fig. 1
Photographs of patient before surgery
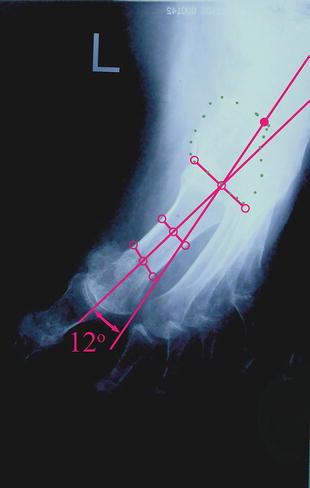
Fig. 2
Metatarsus adductus = 12°
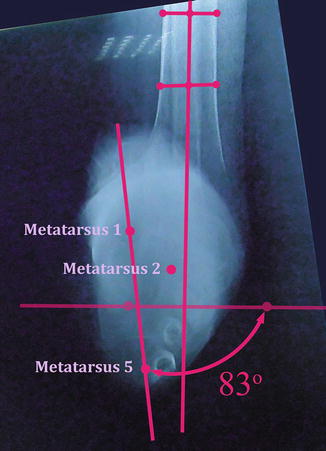
Fig. 3
Forefoot pronation = 83°
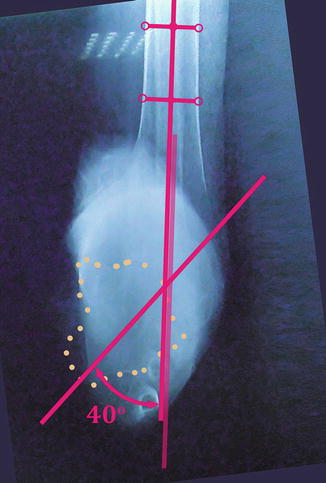
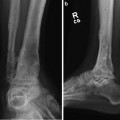
Fig. 4
Calcaneal-tibial angle (frontal plane) = 40° (varus)
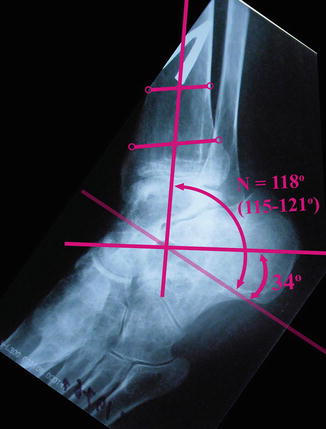
Fig. 5
Calcaneal-tibial angle (sagittal plane) = 34° (dorsiflexion deformity)
3 Preoperative Problem List
There is a complex (midfoot and hindfoot) multiplanar deformity of the left foot:
1.
Metatarsus adductus = 12°.
2.
Forefoot pronation = 83°.
3.
Calcaneal-tibial angle (sagittal plane) = 34° (dorsiflexion deformity).
4.
Calcaneal-tibial angle (frontal plane) = 40° (varus).
5.
Ankle joint arthrosis.
6.
Left-sided spastic hemiparesis.
4 Treatment Strategy
Dissection of plantar fascia, partial Achilles lengthening, acute partial midfoot correction, calcaneal osteotomy.
Applying external fixation for gradual deformity correction.
Hindfoot deformity correction should include 11 mm of distraction, 40° of varization, 18 mm of bringing down, and 10° of dorsiflexion. Total period of correction is 46 days (calculated by software).
Pantalar arthrodesis of the foot (ankle and triple joint fusion) with internal fixation.
5 Basic Principles
“Soft” (not rigid) deformity of the midfoot allows for an acute partial correction of the deformity. After that, the residual deformity is corrected using external fixation.
Osteotomy followed by gradual deformity correction should be made for a rigid hindfoot deformity.
Use of computer-assisted hexapod (Ortho-SUV Frame) provides precise, one-step gradual multiplanar deformity correction.
Because the left-sided spastic hemiparesis confers a high probability of recurrence and the ankle joint has arthrosis, a pantalar arthrodesis of the foot should be done.
6 Images During Treatment
See Figs. 6, 7, 8, and 9

Fig. 6
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
