7 Conservative Treatment
Summary
The most common causes of nasal septal perforation (NSP) are traumatic, postsurgical procedure, inflammatory diseases, and substance abuse. Between 1 and 39% of patients with NSP do not experience any symptoms and are diagnosed during a routine ENT (ear-nose-throat) examination. Conservative managements include nasal irrigation with isotonic saline, application of antibiotic and/ or vitamin ointment, or prosthesis such as a septal button. Surgical procedures are indicated when conservative treatment failed. This chapter focuses on the conservative management as a first-line treatment for those symptomatic cases, leaving surgical repairs for those who do not respond to conservative management.
7.1 Introduction
Nasal septal perforation (NSP) can occur by multiple etiologies, including previous trauma, iatrogenic, inflammatory diseases, substance abuse (e.g., cocaine), use of nasal spray, and others. The prevalence is believed to be approximately 1%; however, 39% of the patients remain asymptomatic until incidental diagnosis in a routine ENT examination. Although most patients with NSP remain asymptomatic, some suffer from bothersome symptoms such as epistaxis, crusting, sensation of nasal obstruction, pain, or discomfort—mostly associated with large perforations. The patients who are in the symptomatic group should initiate with a conservative treatment. If nasal moisture is preserved, the septal perforation is usually asymptomatic. Conservative managements include nasal irrigation with isotonic saline, application of antibiotic and/ or vitamin ointment, or prosthesis such as a septal button. If, despite this conservative management, patients still have bothersome symptoms that affect their quality of life, more aggressive treatments such as surgery can be proposed.
7.2 Pathogenesis
The nasal cavity receives its arterial supply from multiple branches that originated from both the internal and external carotid arteries. Of importance are the branches from the sphenopalatine, along with the superior labial artery, anterior ethmoidal artery (AEA), and greater palatine artery that nourish the Kiesselbach plexus, and therefore the anterior portion of the nasal septum, where most bleeding and perforation occur. 1 , 2 , 3 , 4 , 5 , 6
A chemical or physical damage to the normal anatomy can lead to ischemic necrosis of the septal cartilage, resulting in perforation. Any healing result around the borders of the perforation over the three layers, cartilage, and the two sides of the mucoperichondrium is probably to be thin and atrophic. Therefore, if the edges of the perforation do not heal normally, it gets covered with an atrophic layer of mucosa, producing formation of crusts and a tendency toward bleeding because of the friction of abnormal airflow forces. The turbulent abnormal air forces friction, and the mechanical peeling to relieve a sensation of congestion may result in ongoing crusting, bleeding, and enlargement. 7
When the septum is perforated, the inspired airflow going uniformly over the nasal turbinates adding heat and moisture to the air is disrupted. The inspired air loses its normal airflow pattern through the nasal cavity and begins to recirculate, producing excessive drying of the nasal mucosa that leads to its symptoms.
7.3 Symptoms
Despite being relatively uncommon, NSP has a varying presentation that may imitate pathologies such as septal deviation, allergic rhinitis, and, particularly, chronic rhinosinusitis, with which it may frequently coexist. 8 The patient perception of the symptoms may be influenced by the location and size of an NSP. 9 Diamantopoulos II and Jones 2 found that 92% of NSPs and ulcerations were located anteriorly and 8% were found posteriorly, and that those posterior lesions were frequently associated with trauma or systemic disease such as connective tissue disorders, neoplasia, and syphilis, whereas the anterior ones were associated with trauma and more symptomatic with bleeding and crusting.
The symptom most commonly reported by the patients was bleeding (58%), followed by crusting (43%), nasal obstruction (39%), pain (17%), and whistling (10%), with 15% being entirely asymptomatic, being whistling more often associated with a smaller NSP. 10 In larger NSP there is a great disturbance in laminar airflow and turbulence producing damage and drying of the respiratory epithelia; consequently, more rhinorrhea occurs as the nose attempts to improve the humidity. Turbulence may also create a nasal blockage sensation, which may lead to complications as the patient attempts to remove crusting by manual picking to improve congestion. 9
Therefore, depending on the symptoms suffered by the patient will be the type of treatment recommended.
7.4 Conservative Treatment
The need for treatment depends on whether the patients have symptoms and indeed asymptomatic patients generally do not require any intervention. Underlying cause of septal perforation should be investigated before any intervention is taken. Consider the prevention of septal perforations in high-risk individuals (e.g., cocaine users). 11 , 12
7.4.1 Saline Irrigation
Nasal douches are used in a variety of paranasal sinus diseases such as allergic rhinitis, chronic rhinosinusitis, follow-up treatment in paranasal sinus surgery, prevention in patients with recurrent nasal infection, and dry nose. 13 , 14
According to the evidence, possible mechanism of action that improved mucosal function is due to a direct physical cleaning by irrigation of mucus, crusts, allergens, and debris, eliminating inflammation mediators, and improving the mucociliary clearance by enhancing the ciliary beating rate. 15 , 16 , 17 , 18
Many different kinds of systems display into the market such as wash bottles (sinus rinse), Neti Pot, 60-cc catheter tip syringe, and baby bulb syringe. It can be found in many types of presentations, starting with the type of saline solution that goes from isotonic to hypertonic or the one that can be made at home. In general, most of them are isotonic solutions. Hypertonic saline irrigation not only acts on removing nasal secretions and crusting but also produces reversible cilia stasis, be it in vitro bactericidal and synergic with antibiotics. Osmotic pulls out edema from mucosa and may thin secretions.
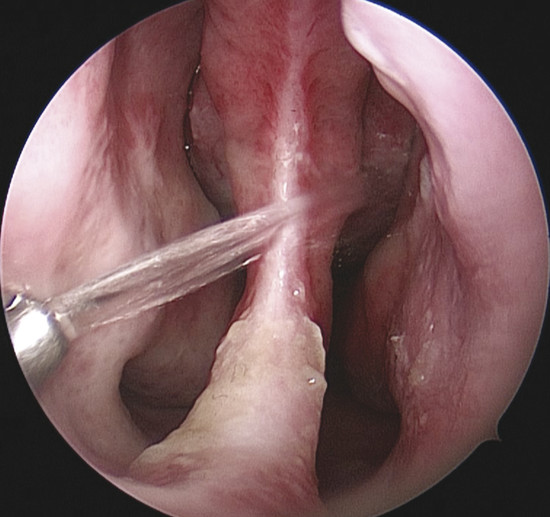
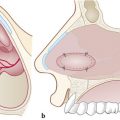
Nasal irrigation can also have different pressures for every requirement (Fig. 7‑1). Those with low-flow volume go out nebulized allowing a soft cleaning and humidification of the nasal cavity, preferring as a maintenance therapy when there is no much secretion and crusts. The medium-flow volume is recommended when wanting a thorough cleaning or there are some crusts, leaving the high-flow volume for severe crusting and secretions. For irrigation of the whole nasal cavity, compressible douching systems that have a minimum output pressure of 120 mbar, a good connection of the outlet to the nostril, and irrigation stream that is directed upward (45 degrees) are recommended (Fig. 7‑2). Moreover, the material should be transparent, easy to clean, and disinfect, and should not contain harmful elements. 18

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


