7 Cleft Palate Repair
Introduction
Repair of the cleft palate serves to restore the separation between the oral and nasal cavities—creating a functional velopharyngeal mechanism for feeding, speech, and eustachian tube (ET) function—with the intent of minimizing the repair′s impact on maxillary growth. This serves to facilitate oral feeding and verbal communication. Most often, cleft palate is an isolated finding, but > 30% may have an associated syndrome and/or comorbidities. Appropriate evaluation, education, and counseling in conjunction with the primary care provider and the entire cleft and/or craniofacial team is important in the perinatal period to ensure that families understand how to feed and care for their child with a cleft palate.
Surgical goals must be kept in mind when evaluating candidacy and timing of repair as well as when providing counseling to family. Expectations and counseling are catered to the individual. The presence of comorbid conditions (congenital cardiac disease, neurodevelopmental disorders, concurrent aerodigestive tract anomalies) can jeopardize surgical candidacy, affect overall prognosis, and/or compromise surgical outcomes.
Airway Evaluation and Management
Obstructive sleep apnea (OSA) and sleep-disordered breathing (SDB) can be common comorbidities in children with cleft palate. Features of children with cleft palate that can contribute to OSA and/or SDB include hypoplastic mandibular and midfacial development (either developmental or related to scarring from surgical repair of cleft palate), presence of concurrent syndrome, and/or hypotonia. OSA or SDB can affect the timing of surgical intervention and increase postoperative risk. Robison et al.1 reported a prevalence of OSA of 8.5% in the cleft populations at an average age of 5 years old, but some were identified at an earlier age, which is significantly higher than 2 to 3% in the general pediatric population. Despite its prevalence, OSA remains an underrecognized entity in the multidisciplinary cleft clinic. Using a validated questionnaire to identify OSA in cleft patients < 5 years of age, MacLean et al.2 identified that although 31.4% of the responders had patients with features consistent with moderate to severe OSA, only 30% of symptomatic patients had a polysomnogram to evaluate their sleep disturbance.
Muntz et al.3 reported a 22% rate of sleep disturbance within his cleft population, and within the 57% of patients with SDB that received polysomnography (PSG), 88% had mild to severe OSA. Syndromic children were more likely to have SDB and also undergo PSG than their nonsyndromic counterparts. These data suggest that patients with cleft palates are more at risk for OSA before and after cleft palate repair, and continued vigilance for airway obstruction is required over their course of care. If OSA is suspected before cleft palate repair, a sleep study should be obtained and, if OSA is present, discussion with the family about potential worsening of OSA after cleft palate repair is important as well as potential observation in the intensive care unit (ICU) after surgery.
Given that both cleft and OSA carry an independent association with neurodevelopmental delay, it is important to carefully screen and manage sleep disturbance in this at-risk population.
Immediate postoperative airway obstruction has been reported to affect 5.7% of patients undergoing palatoplasty.4 This risk is higher in patients with a syndrome or with Pierre Robin sequence. Administration of perioperative dexamethasone has been shown to decrease postoperative airway obstruction without adverse consequences on wound healing.5
The authors often place a midline 2-0 silk tongue suture to be removed prior to leaving the postanesthesia care unit. This maneuver assists with airway optimization during emergence from anesthesia while minimizing risk to the surgical repair site. Surveillance with continuous cardiorespiratory monitoring is performed throughout the patient′s hospitalization. In rare circumstances, initiation of supplemental oxygen or noninvasive positive pressure ventilation is necessary, which may be continued into the postoperative period. Augmentative airway support is more likely in patients with micrognathia, hypotonia, or other conditions that affect the airway and may warrant observation in the ICU.
Surgical repair has been demonstrated to be a risk factor for development of OSA, necessitating OSA surveillance during the postoperative period. Mild OSA was identified in all patients in a small cohort undergoing Furlow palatoplasty for velopharyngeal insufficiency (VPI).6
As cleft palate repair can worsen preexisting OSA, it is important to have a management plan in place prior to surgery. Risk stratification begins at the new patient evaluation. The surgeon should assess for signs and symptoms of sleep disturbance, obstructive/cyanotic events, feeding/aspiration issues, weight gain, and the need for recurrent hospitalizations. Positive findings should be further evaluated with flexible fiberoptic laryngoscopy, occupational therapy evaluation, and/or microlaryngoscopy and bronchoscopy. Based on the flexible upper airway exam, surgery to address tongue or laryngeal airway obstruction can be performed. While clinical judgment is paramount in the evaluation of these children, PSG may help stratify the severity of OSA and guide preoperative interventions and timing of surgical repair. Evaluation by pediatric pulmonology, pediatric cardiology, and genetics may help define other congenital anomalies.
Classification
The Veau classification is the most popular classification system, separating cleft palate into four groups:
Group I: defect of the soft palate only
Group II: defect involving both the hard and soft palate
Group III: defect involving the hard and soft palate and alveolus
Group IV: bilateral complete cleft palate
Not included in this grading system is submucous cleft palate (SCP), a small subgroup of patients with cleft palate. Its incidence is far more rare than clefts of the secondary and primary palate, reported as 1:10,000 to 1:20,000 by Ysunza et al.,7 but this could be related to an underdiagnosed and often asymptomatic subpopulation. McWilliams et al.8 reported that 44% of 130 patients with SCP did not require surgical intervention based on speech assessments.
SCP is defined by a discontinuity of palatal musculature at the midline with mucosal continuity. Hallmark signs include a hard palatal notch, bifid uvula, and a zona pellucida, representative of midline muscular discontinuity. Although at least some of these findings are present in most patients, the presentation may be quite subtle and easily missed without a high index of suspicion.
Patients with occult SCP lack these characteristic findings, but do have anomalous insertion of the levator veli palatini (LVP) onto the hard palate. This was characterized by Stal and Hicks9 in three types: A, major portion of velar musculature inserts onto hard palate; B, moderate portion inserts onto hard palate; C, minimal portion inserts onto hard palate. Endoscopic examination and surgical intervention has been used in the past to identify these variations; however, most recently, magnetic resonance imaging has been shown to be useful in identifying occult SCP in order to determine if patients require surgical repair versus continuity of speech therapy.10
Timing and Patient Selection
As cleft palate repair has a deleterious impact on craniofacial growth, timing of repair should be balanced with the impact on speech and language development. Some advocate early repair of the soft palate with delayed hard palate management to avoid impairment of maxillary growth. Sommerlad et al.11 reports success with primary palate repair at the time of lip repair (3 months) with definitive palate repair at 6 months, although Kirschner et al.12 failed to find any difference in speech outcomes in patients repaired at 3 to 7 months of age versus > 7 months of age. The American Cleft Palate-Craniofacial Association currently recommends cleft palate repair by 18 months, and many advocate that repair be done before 1 year of age. At our institution, we perform palate repair at 10 to 12 months, prior to significant speech development.
Comorbid conditions can often delay or preclude surgical repair. As mentioned in the introduction, in the presence of life-threatening comorbidities, such as complex congenital heart disease, pediatric cardiology and cardiac anesthesia consultations are often helpful in determining when the patient would be safe for general anesthesia. Patients with neurodevelopmental delay who are nonverbal and gastrostomy tube–dependent may never benefit from surgical repair.
General Preoperative Considerations
On the day of surgery, the patient is assessed for recent illnesses or hospitalizations. An upper respiratory infection increases perioperative risk and surgical intervention should be postponed. Concerns for hearing loss or middle ear pathology should be pursued with exam, under anesthesia, of ears with possible myringotomy with tube placement.
Orotracheal intubation may be challenging in patients with craniofacial anomalies such as midface hypoplasia and micrognathia and will likely need to be observed in the ICU postoperatively. It is imperative that the surgical team communicates with anesthesia regarding previous physical exam, flexible fiberoptic laryngoscopy findings, and developing a clear plan for airway management. Once orotracheal intubation is achieved, typically with an oral right angle endotracheal tube, it is secured in the midline of the lower lip.
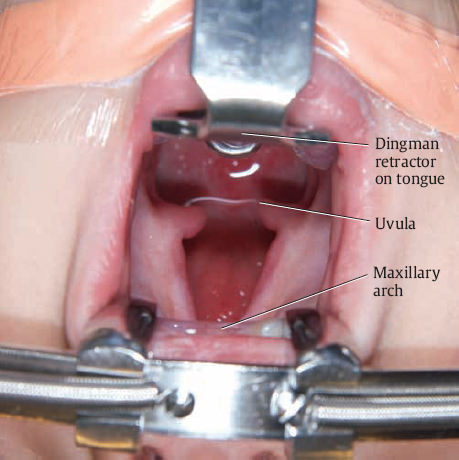
The patient is positioned in gentle cervical extension, if there are no contraindications, and suspended with the Dingman retractor. The two teeth hooks are adjusted throughout the duration of the case depending on the region of the anterior palate in need of exposure. The lateral cheek retractors gain additional visualization. The authors use the LightMat (Lumitex Medical Devices, Strongsville, OH) for intraoral illumination rather than a surgical headlight; both are adequate for intraoperative visualization. Loupe magnification is used (2.5×). The hard palate, soft palate, and general site of the neurovascular bundle are injected with 0.5% lidocaine with 1:200,000 parts epinephrine. Injection/surgical planning is performed prior to draping, allowing for adequate vasoconstriction. Some surgeons advocate oral preparation with chlorhexidine mouthwash, diluted hydrogen peroxide, or povidone-iodine solution, and these preparations have been demonstrated to decrease oral flora. However, presence of positive cultures in the throat has been shown to have no impact on the postoperative fistula rate.13 The authors have found no benefit and therefore do not use any oral preparation prior to surgery.
Surgical Techniques
As each cleft palate is morphologically unique, the surgical technique that one selects should cater to the alveolar, hard palatal, and soft palatal deficits that are identified. It is not uncommon to integrate components of several types of palatoplasty in order to achieve the goals of oronasal separation, restoring a functional velopharyngeal mechanism, with attention directed to minimizing the impact on maxillary growth.
Technique selection begins with careful examination. Width of the hard and soft palatal clefts, width from the medial edge of the cleft to the alveolus, exposed vomer, width of the alveolar cleft, approximation of the soft palatal cleft with the posterior pharyngeal wall, viability of tissue, and presence of other comorbidities that may place the patient at risk for OSA are critical in deciding which techniques are necessary to achieve functional goals. These metrics should be recorded along with photo documentation.
The principles of palatoplasty are:
A tension-free closure
Repositioning of the velar muscles
Multilayer closure
Despite the variable morphology of cleft palate defects, honoring these principles will ensure an optimal surgical repair.
The main techniques of palatoplasty that are discussed include:
von Langenbeck palatoplasty
Two-flap palatoplasty
Furlow palatoplasty
The Children′s Hospital of Philadelphia (CHOP) modification of the Furlow palatoplasty
These techniques, among their many described modifications in the literature, offer a comprehensive repertoire for palate repair. In addition, the use of vomer flaps in bilateral clefts and intravelar veloplasty (IVV; complete release of the levator musculature and posterior rotation) are complimentary, yet critical maneuvers to achieve functional, tension-free, multilayer closure. It is important to consider the width of the cleft when determining whether to incorporate a Z-plasty as part of the cleft palate repair.
Von Langenbeck Palatoplasty
Flap Design
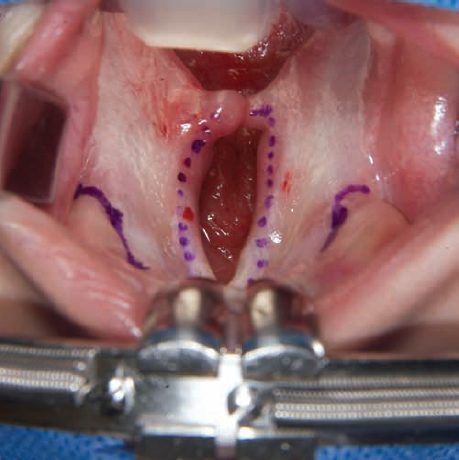
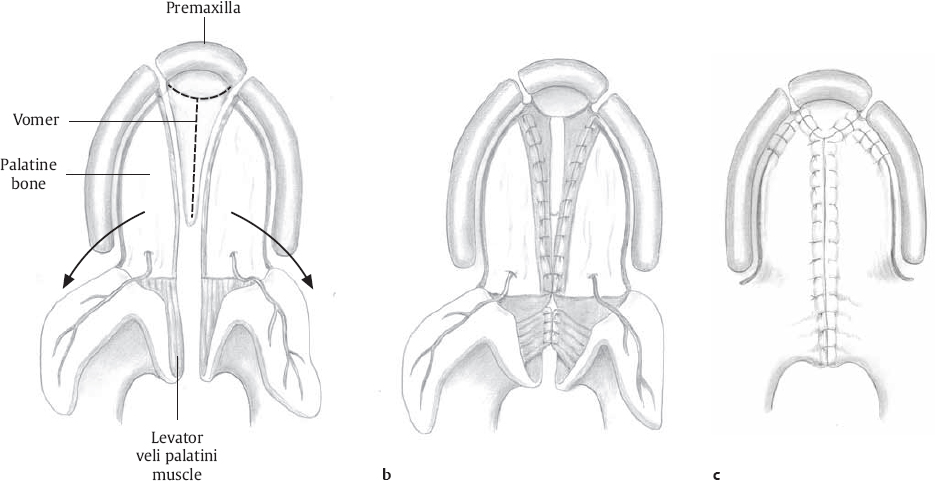
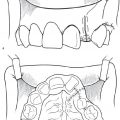
This begins with lateral-releasing incisions around the alveolar ridge that preserve anteriorly and posteriorly based flaps and spare the gingiva laterally ( Figs. 7.1 and 7.2 ). Approximately 1 cm of anterior pedicle should be preserved in the case of a cleft of the secondary palate; this can be brought to 0.5 cm from the margin of the alveolar cleft in cases of complete cleft. This can be carried laterally around the posterior extent of the alveolus for additional mobilization.
Medial cleft edge incisions are oriented at the oral/nasal mucosal junction and carried posteriorly to the apex of the uvula. Incisions along the bony margin are made with no. 15 blade, with soft palatal and uvular dissection with a no. 12 blade.
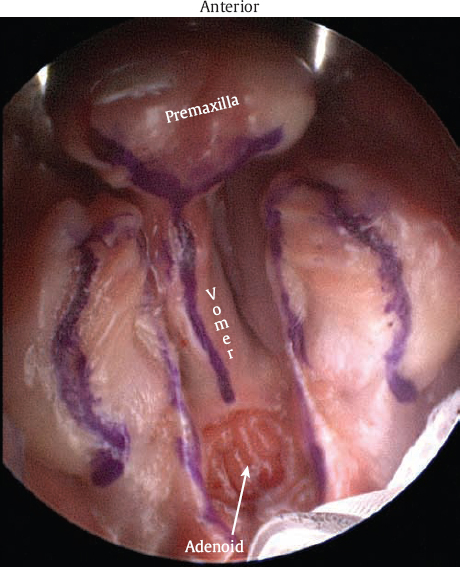
Incorporate exposed vomer into flap design. Nasal and vomer flaps are far less robust than their oral counterpart, so tension-free closure is critical. Vomer flaps can be elevated to the skull base, providing generous length in unilateral or bilateral repair. The location of the vomer incision can be symmetrical or asymmetrical and should be catered to the orientation of the vomer with respect to the cleft and the length of nasal flaps. Therefore, vomer flaps can be recruited to compensate for short nasal flaps. The flaps terminate at the posterior limit of the vomer.
Elevation of Hard Palate Flaps
Submucoperiosteal dissection is carried laterally to medially and brought in continuity with the medial cleft edge incision with a Joseph elevator. Medial dissection should be freed anteriorly at the alveolar ridge and posteriorly at the hard/soft palate junction.
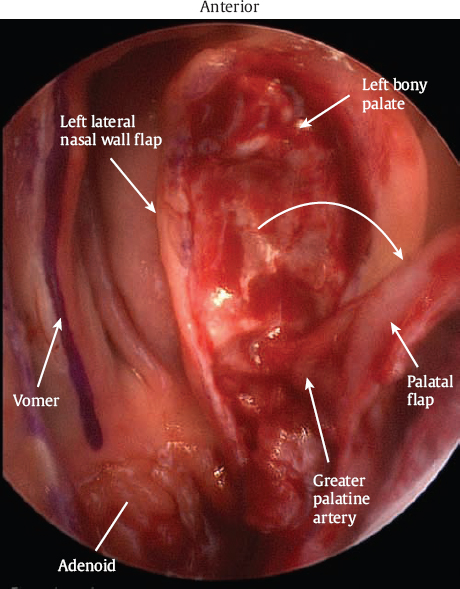
Blunt elevation in the submucoperiosteal plane to the posterior edge of the palate will allow for atraumatic identification of the greater palatine neurovascular bundle.
Free the greater palatine neurovascular bundle in a 360-degree fashion. This can be done with an angled gingival separator. Additional length can be gained with dissection of the pedicle with a no. 12 blade or an angled dissector behind the pedicle, separating proximal pedicle from its insertion along the flap. This procedure can threaten the pedicle and so should be done with careful consideration. Alternatively, the pedicle can be osteotomized from the posterior bony foramen to gain length, but it also threatens the pedicle.
Hemostasis is generally self-limited and can be encouraged with oxymetazoline pledgets; bipolar cautery should be performed with protection of the neurovascular pedicle.
Elevation of Nasal Flaps
Submucoperiosteal dissection is then carried along the lateral nasal wall to the undersurface of the inferior turbinate with a Cottle elevator or other angled elevator.
Approximation with the adjacent vomer flap will dictate the extent of elevation needed for tension-free closure.
Intravelar Veloplasty: Dissection of Muscle Flaps
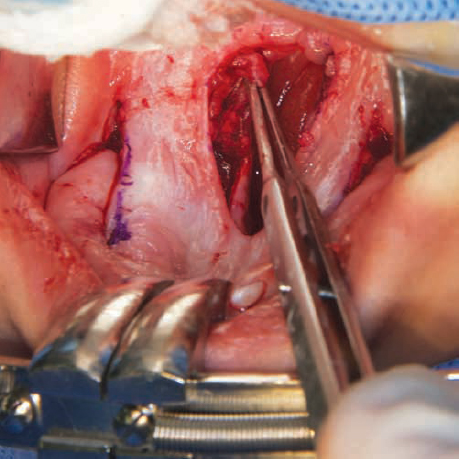
Nasal submucosal dissection is now performed along the posterior edge of hard palate, releasing the LVP from its anomalous insertion at the hard/soft palatal junction ( Fig. 7.3 ).
Elevation should continue laterally behind the greater palatine neurovascular bundle to the hamulus.
This will not only reorient the LVP but will gain additional length for both mucosal and muscular layers.
Nasal Closure
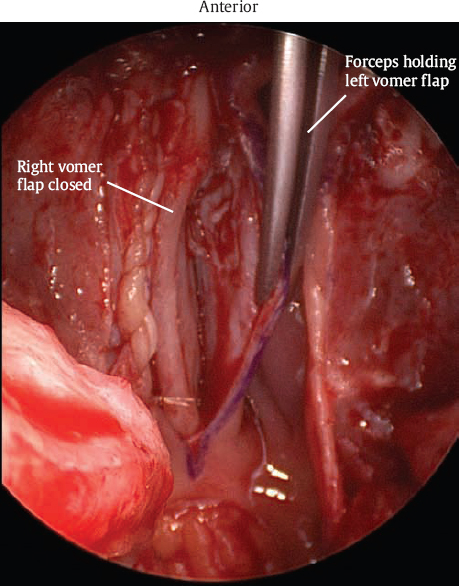
Interrupted 5-0 Monocryl (Ethicon, Somerville, NJ) sutures are placed in a mucosal to submucosal fashion in order to orient knots along the nasal surface and evert the edges of the nasal mucosa.
The apex of the uvula is oriented with a horizontal mattress 5-0 Monocryl suture.
Closure proceeds in a tension-free fashion, incorporating vomer flaps anteriorly.
Intravelar Veloplasty: Unity of Muscle Flaps
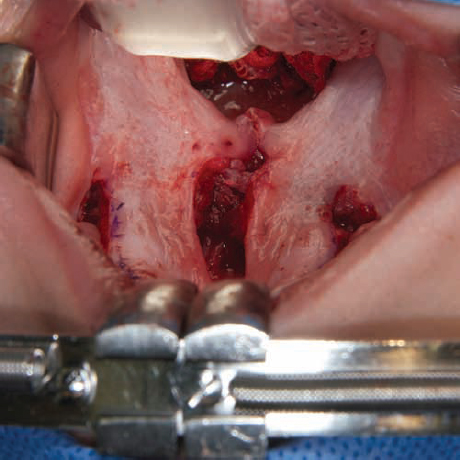
Interrupted or horizontal mattress sutures of 4-0 polydioxanone are used to orient the LVP along the posterior velum. Only two or three of these deep sutures are usually necessary to confer strength of closure, and allow for less suture tension on the oral mucosal closure ( Fig. 7.4 ).

Oral Closure
Interrupted 5-0 Monocryl sutures are placed approximately every 3 mm in posterior to anterior fashion.
Lateral Stay Sutures
The relaxing incisions are stabilized with interrupted 5-0 Monocryl sutures through the medial gingival edge.
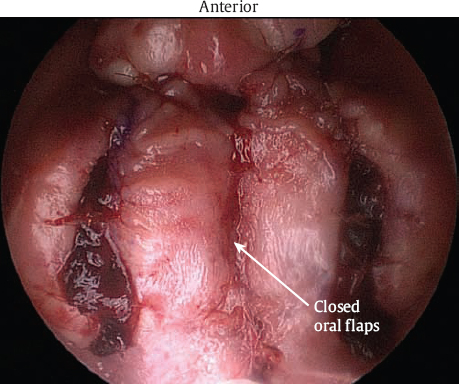
Surgicel (Ethicon), or comparable resorbable packing, is placed in these lateral recesses to obliterate dead space; their displacement is prevented with the stay sutures. Most often these are tied with loose air knots to stabilize, but not necessarily approximate, the edges of the relaxing incisions ( Fig. 7.5 ).
Two-Flap Palatoplasty
Flap Design
Similar to the von Langenbeck palatoplasty, lateral-releasing incisions are planned along the alveolar ridge but are now carried anteriorly to the cleft margin. As in the von Langenbeck palatoplasty, mucosal incisions are made with no. 15 and 12 blades. In some instances, a 60-degree angled Beaver (no. 6910) blade, is used to make incisions at the most anterior limit of the palate and along the anterior cleft edge ( Fig. 7.6 ).
Alternatively, in patients with a unilateral cleft, mucoperiosteal disturbance can be minimized with elevation of the noncleft-side flap and not the lateral aspect of the cleft-side flap in narrow clefts (< 10 mm). A variation of this was described by Furlow (below). The flap is then anteriorly and laterally based as the gingival/palatal junction i ncisions are not made. Closure of the cleft in this scenario relies upon:
Excellent mobility of the noncleft-side palate flap
Medial dissection of the cleft-side palate flap to gain width by losing height of the palatal arch
Vomer flaps:
In cases of bilateral cleft palate ( Figs. 7.7 , 7.8 , 7.9 , 7.10 , and 7.11 ), the vomer flap can be oriented at the apex of the vomer to facilitate closure with its adjacent lateral nasal wall mucoperiosteal flap.
The vomer flap in a unilateral cleft palate is typically incised along its junction with the noncleft-side palate flap and is rotated toward the cleft side to join the nasal mucoperiosteal flap or cleft-side palate flap. Pichler14 first described this for the management of wide cleft and referenced in Furlow′s description of double opposing Z-palatoplasty. Sommerlad et al.11 advocates use of this vomer flap for a single-layer closure at the time of lip repair, typically 3 months.
Flap Elevation on the Hard Palate
Submucoperiosteal dissection is carried anteriorly to posteriorly, with identification of the greater palatine neurovascular bundle.
This can be done on both sides in the traditional Bardach et al.15 two-flap palatoplasty. As described above, the noncleft-side flap is elevated in the standard fashion, with the neurovascular pedicle skeletonized to facilitate mobility. The cleft-side flap is then elevated at its medial border only. An additional benefit of this technique is that if closure is not possible, it can easily be converted to the standard two-flap Bardach procedure.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


