Fig. 1
Pre-operative clinical photo. Anterior view

Fig. 2
Pre-operative clinical photo. Medial view

Fig. 3
Pre-operative clinical photo. Lateral view

Fig. 4
Pre-operative clinical photo. Plantar view

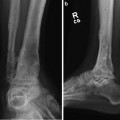
Fig. 5
Pre-operative AP view of the ankle

Fig. 6
Pre-operative lateral view of the ankle
3 Preoperative Problem List
Deformity analysis:
20° plantar flexion deformity
15° cavus deformity
10° pronation deformity
CORA for midfoot cavus deformity located at the apex of the deformity at the dorsal talonavicular joint
CORA for ankle equinus located at the lateral talar process/center of rotation of the ankle
Previous surgeries plus her condition have resulted in very stiff, noncompliant soft tissues. Acute correction is not possible.
4 Treatment Strategy
Gradual correction was chosen and the treatment of choice due to the failure of previous acute corrections. In addition, the soft tissues were stiff and noncompliant. Acute corrections utilizing osteotomies and soft tissue releases have failed in the past. Fusions are not indicated in patients with open growth plates. The best way to maintain her joints and still obtain adequate corrections is to utilize gradual correction. One could perform a combination of midfoot and hindfoot osteotomies and gradually correct through these osteotomies. In this case it was felt that a pure soft tissue correction through the patient’s midfoot and hindfoot joints would provide adequate correction through remodeling of her soft tissues and bone structure.
The Taylor Spatial Frame was chosen to perform a two-stage correction. A butt frame configuration was first applied to correct the cavus and pronation deformities. Once this was accomplished, the frame was revised into an equinus frame configuration to address the ankle deformity.
5 Basic Principles
Deformity analysis revealed three deformities: pronation through the forefoot, cavus through the midfoot, and equinus through the ankle. In this case, a pure soft tissue correction with the frame was indicated. No acute soft tissue releases were performed. No bony work was performed as stated above. The origin for the cavus deformity correction was set at the dorsal surface of the talonavicular joint. The structure at risk was set as the plantar skin. A butt frame was applied first to correct the cavus and pronation, allowing her planter skin to stretch at 1.5 mm/day. One centimeter of distraction was built into the midfoot correction to unbind the joints. The frame was then revised to a standard equinus configuration with the origin at the lateral process of the talus and the structure at risk at the skin posterior to the Achilles. The skin was allowed to stretch at 1.5 mm/day. The equinus deformity was overcorrected by 10° to account for expected rebound of her soft tissues after frame removal. Her neurovascular status was monitored closely to ensure that the correction did not result in a tarsal tunnel syndrome. Correction time was 3 weeks for the cavus deformity and 4 weeks for the equinus deformity. The frame was then left in place for 2 months after the correction was completed to ensure adequate time to allow the soft tissues to adjust and remain compliant after frame removal. The patient was placed in to a custom AFO to be worn 23 h per day until she reaches skeletal maturity.
6 Images During Treatment
See Figs. 7, 8, 9, 10, 11, 12, 13, 14, 15, and 16
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
