Fig. 1
AP foot with metatarsus adducts

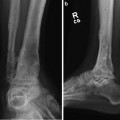
Fig. 2
Lateral foot: flat top talus, subtalar varus

Fig. 3
Erect leg standing radiographs: short left femur (5 mm) and left tibia (25 mm). Mechanical Axis Deviation (MAD): 15 mm Lateral on the left. (Normal MAD: 0–3 mm). Mechanical Lateral Distal Femoral Angle (mLDFA): 82° (Normal range: 85–90)

Fig. 4
Long leg lateral Xray
3 Preoperative Problem List
Limb length Discrepancy: Femur (0.5 cm); Tibia (2.5 cm). Total of 3 cm.
Distal femoral valgus
Equinus ankylosis of 15°
Peroneal nerve at risk
4 Treatment Strategy
Peroneal nerve release
Osteotomy of the femur (multiple holes technique)
Temporary application of external fixator device (fixator-assisted plating)
Internal fixation of femoral osteotomy with locking plate
Tarsal tunnel decompression
Supramalleolar osteotomy of tibia
Application of multiplane hexapod computer-assisted fixator (TSF)
5 Basic Principles
Postsurgical adhesion/scar tissue formation may guide the surgeon to perform gradual correction, while smaller-magnitude deformity in areas of no prior surgery may be treated with acute correction techniques such as opening/closing wedge osteotomies. Utilization of the osteotomy rule principles is helpful in preventing malposition through incorporation of translation when the osteotomy is placed outside the apex of deformity, as with the case presented of equinus contracture where the apex was located at the center of rotation of the ankle and the osteotomy placed proximal at the supramalleolar region. It should also be noted that the acute femoral osteotomy was made proximal to the apex of deformity, necessitating medial angulation and lateral translation of the distal fragment.
6 Images During Treatment
See Figs. 5, 6, 7, 8, 9, 10, 11, and 12.

 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
