6 Transsexualism
6.1 Fundamentals
When a male or female patient presents seeking gender reassignment surgery, the surgeon must ascertain whether the medical and legal requirements for such an intervention have been met. This requires a proper statement of the indication in writing by a psychiatrist or medical psychotherapist experienced in this field. Moreover, this statement must show that the diagnosis of transsexualism has been confirmed and that the requirements according to current standard of treatment have been met.
After a thorough history has been obtained and a complete examination performed, an individualized surgical treatment plan is formulated. Patients must be comprehensively informed, and their informed consent should be obtained well before the date of surgery. They must have a detailed understanding of the postoperative results and possible complications.
Note
Note that in applicable cases the respective health care provider must issue confirmation of cost coverage.
6.2 Male-to-Female Transsexualism
6.2.1 History
The first reports of sex reassignment operations in transvestites in Germany were published as early as the 1920s. Another 30 years passed before the American sexologist Harry Benjamin introduced the distinction between transvestism and transsexualism, a distinction still found today in the ICD-10 classification (the 10th revision of the International Statistical Classification of Diseases and Related Health Problems) under F64.0 through F64.9.
Gynecologist Georges Burou set an important milestone in Casablanca in 1956: he performed the first sex-reassignment genital surgery on a male-to-female transsexual patient. Burou created a vaginal cavity between the bladder and prostate and lined it with an inverted penile skin flap. The patients who successfully underwent surgery in this manner helped this surgical method achieve worldwide recognition. The gynecologists providing aftercare to these patients contacted Burou to study this technique. It was only in the early 1970s that this method came into widespread use in various countries. Since then various aspects of the method have undergone further development. Even today, the penile skin flap inversion vaginoplasty pioneered by Burou still remains the most commonly used method.
6.2.2 Goal of Treatment
The goal of sex-reassignment surgery in the male-tofemale transsexual is to fashion genitals that most closely approximate natural female genitals in their appearance and function. This requires the construction of a neovagina of sufficient depth and width to allow sexual intercourse. Additional requirements include sufficient sensitivity and the capacity for lubrication when sexually excited. The vulva should also include a sensitive clitoris with a prepuce as well as labia majora and labia minora. The external orifice of the urethra must be positioned so that the patient can easily urinate in a seated position.
6.2.3 Sequence of the Surgical Procedures
Various surgical techniques are available for achieving the goals described above, and there are big differences between some of them. However, there is a strong consensus with respect to the sequence of the surgical steps:
Bilateral orchiectomy.
Amputation of the penis with resection of the corpora cavernosa.
Dissection of a neovaginal cavity with a sensitive lining.
Creation of a female urethral meatus.
Construction of a female vulva with labia and clitoris.
Various orchiectomy techniques are possible. These involve exposing the testes and spermatic cords as far as the inguinal canal and then ligating and removing them.
The amputation of the penis involves dissecting the penis out of its skin between the Colles fascia and Buck′s fascia. Then the glans is exposed and mobilized, taking particular care to spare the dorsal neurovascular bundle. The neurovascular bundle is either dissected under magnification (binocular loupe) or a strip of erectile tissue is left in situ to protect it. The urethra is isolated from the corpora cavernosa along the base of the penis, divided at skin level, and circularly sutured into the inverted penile skin. Depending on the specific technique, the corpora cavernosa are removed either to a certain depth or even completely.
The dissection of the neovaginal cavity begins over the central tendon, the fibrous midpoint of the perineum. This structure forms the junction of the bulbocavernosus, sphincter ani externus, levator ani, and transverse perineal muscles. After dividing the central tendon, the surgeon then dissects the neovaginal cavity in the rectovesical pouch posterior to the prostate between the two sheets of Denonvilliers’ fascia.
The following options are available for lining the vaginal cavity:
Inversion of the penile skin.
Inversion of the penile skin in combination with a free skin graft.
Inversion of the penile skin in combination with pedicled procedures.
Other options, such as pedicled bowel segments and various flaps (free or pedicled).
In the simple inversion technique, the penile skin is inverted and used to form the lining of the neovagina. Placing tension on the penile skin alone is not enough to create a vagina of sufficient depth; this also requires mobilizing the mons pubis and the skin of the lower abdomen. This creates significant tension in the midvulvar region over the pubic symphysis. Deep retention sutures, which may be placed laparoscopically, and fibrin glue are recommended to minimize the risk of postoperative prolapse. In spite of this, retrograde migration and even complete prolapse of the penile skin is relatively common in the postoperative phase.
The tension on the penile skin often creates an undesirable midline indentation in the mons pubis. Construction of a clitoral hood and labia minora is technically difficult with this method and as a result it is often not attempted in the primary procedure. When the scarring process has run its course about 6 months postoperatively, a monsplasty can be performed to correct the midline indentation in the mons pubis, and a prepuce can be fashioned to cover the clitoris. This second step often requires deepening the vaginal introitus as well. One will encounter difficulties using this method in a circumcised patient or one with a small penis, which is why additional skin grafts are recommended.
Free skin grafts from the genital region are primarily scrotal skin grafts, which can be harvested without creating an additional donor-site defect. Split-thickness skin grafts have been shown to exhibit an excessive strong tendency to shrink. For this reason, full-thickness skin grafts should usually be preferred. The urethra can also provide tissue for a local flap. Instead of being shortened to skin level, it can be split open lengthwise where indicated and integrated into the inverted penile skin. This makes it possible to lubricate the vagina. Where there is not enough penile skin available, one can achieve sufficient depth in the vagina by using the scrotal skin to create a posteriorly pedicled scrotal flap.
Because of their surface texture and available length, pedicled bowel flaps are often suggested as a lining for the neovagina. Given the greater invasiveness of an additional intra-abdominal intervention and the possible complications it entails, most surgeons no longer perform this type of operation as a primary procedure. Other pedicled flap procedures such as the pudendal thigh flap or medial thigh flap have failed to gain widespread popularity because of their donor-site morbidity and flap thickness.
The clitoris is fashioned from the glans. This can be done by partially deepithelializing the glans and reducing its size. It can then be fixed as a pedicled flap above the reconstructed urethral meatus.
The labia majora are created from the residual lateral scrotal skin. The soft tissue can be mobilized to provide additional subcutaneous substance.
Combined Method According to Schaff and Morath
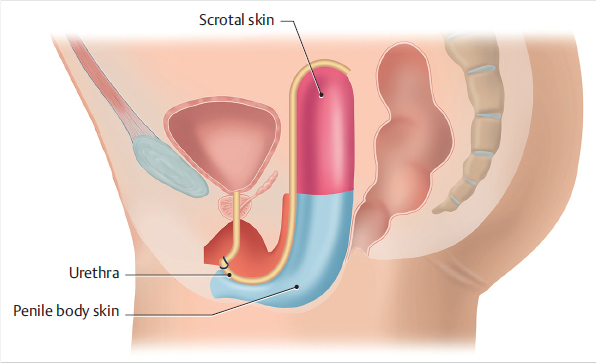
In light of the complexity of genital surgery in male-tofemale transsexuals and the lack of a uniform surgical method, Schaff and Morath have combined the surgical components in such a manner that an optimal functional and aesthetic result can be achieved for the patient. The procedure of this standardized combined method is described below. We can begin by noting that the term “combined method” has been chosen because the vaginal lining is composed of a combination of different types of skin (▶Fig. 6.1).
6.2.4 Preparation for Surgery
After consultation with the attending endocrinologist and after assessment of the risk of thrombosis in the specific case, the estrogens are decreased or discontinued accordingly prior to surgery. In the preoperative consent discussion conducted after the initial consultation, the surgeon again explains the surgical technique and informs the patient of the possible risks and complications. Aside from the general risks of surgery such as infection, bleeding, impaired wound healing, and decubitus lesions, the following aspects must be given particular emphasis:
Necrosis due to reduced perfusion.
Nerve injuries and sensory deficits in the clitoris resulting from injury to the neurovascular bundle.
Injury to adjacent internal organs, especially the bowel, bladder, and urethra with resulting fistulas.
Failure of the skin graft to heal in place.
Shrinkage of the neovagina.
Meatal stenosis.
Need for surgical correction.
The patients are admitted to the ward 1 day prior to surgery. In addition to the routine preoperative diagnostics, the patients receive a thorough bowel prep to minimize the risk of infection or secondary fistula formation in the event of a bowel injury requiring a suture.
6.2.5 Positioning
Patients are positioned on the operating table supine with the legs abducted. For the dissection of the vaginal cavity, they are placed in a head-down position. The legs are not placed in the lithotomy position so as to avoid injury to the superficial peroneal nerve and also to avoid compartment syndrome. This is important in a procedure that lasts, on average, 3 to 4 hours.
6.2.6 Surgical Technique
The sex-reassignment operation has two objectives:
Creation of a sensitive, lubricating, and sufficiently deep neovagina.
Construction of a neovulva.
The best functional and cosmetic result is achieved when three different types of skin are used in combination for lining the vaginal cavity. The inverted penile skin is used for the vaginal introitus. As this is used only from the region of the introitus, it neither requires undermining the abdominal skin, which risks injury to cutaneous sensory nerves, nor creates tension over the pubic symphysis. This means that the mon pubis remains completely natural and unscarred. This largely eliminates the risk of vaginal prolapse and, with it, the need for additional deep sutures.
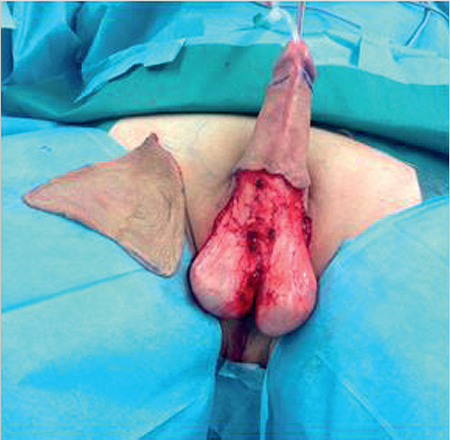
The combined method does without a posterior scrotal flap, keeping the introitus free of hair and avoiding an aesthetically unappealing funnel-shaped introitus. Therefore, the scrotal skin is used as a free skin graft deep within the vaginal cavity. The skin is harvested before the orchiectomy (▶Fig. 6.2) and thinned prior to placement so that nearly all hair follicles will have been removed. The scrotal skin can be harvested without creating an additional donor-site defect or scar, making it preferable to any other free skin graft. In patients with a small penis and scrotum which do not provide enough skin, an additional free skin graft can be harvested from the medial thigh.
One important aspect is the vagina’s ability to produce lubrication. Experience has shown that penile and scrotal skin alone cannot provide this. As the urethra is practically ideal for this purpose, it is not resected. To avoid endangering the perfusion of this long narrow flap, the urethral erectile tissue (corpus spongiosum) is initially left fully intact. It can later be reduced if necessary. This technique achieves a sufficiently large lining for the vagina, regardless of the size of the penis or whether the patient is circumcised. The neovaginal cavity is dissected as far as the peritoneum, as described above.
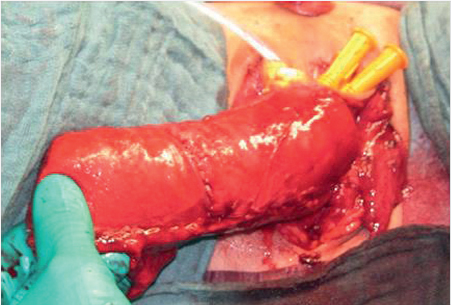
The vagina is then constructed outside the body by splitting the penile skin longitudinally, inverting it over a foam rubber stent, and suturing it to the split urethra. The greatly thinned scrotal skin is sutured to the distal end to complete the vagina (▶Fig. 6.3). Only now is the neovagina inverted into the neovaginal cavity.
The clitoris is fashioned from the dorsal portions of the glans and coronary groove. Here, there are about as many nerve endings as around the highly sensitive urethral meatus. The inner surface of the prepuce is split; both parts remain highly sensitive and well perfused so they can be used for fashioning the labia minora. The entire dissection is performed under optical magnification.
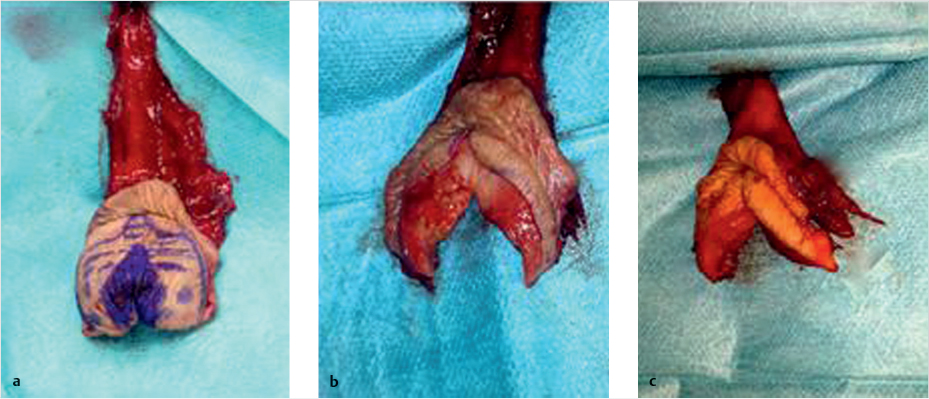
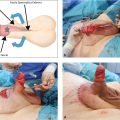
Once the penile skin has been inverted without tension, a central Y-shaped skin incision is made at its base. The neurovascular structures beneath it are dissected in two layers. The glans, now reduced to a clitoris, can be sutured to the inner layer of the prepuce through this incision (▶Fig. 6.4a–c). In this manner, the entire complex of prepuce, clitoris, and labia minora is created in the primary procedure. The result is a clitoris with a natural appearance and protective hood just like its biological counterpart.
6.2.7 Postoperative Bandage
Two or three disposable female catheters are inserted into the foam rubber stent lying within the neovagina at the end of the operation. The catheters press the tightly rolled stent apart, increasing the pressure on the full-thickness skin graft. However, this pressure is not sufficient to endanger the pedicled urethral epithelium or the inverted urethra.
The clitoris–labia complex is gently maintained in its ideal shape with the aid of small foam rubber wedges. The wedges are also fixed in place with temporary sutures (▶Fig. 6.5). A foam rubber pad is fixed over the vulva to prevent swelling or displacement. This is also done to ensure that the patient can be mobilized immediately.

6.2.8 Postoperative Phase
Postoperative perfusion of the clitoris and labia minora is monitored daily. If venous stasis or reduced perfusion is detected, the sutured foam rubber wedges will be removed immediately. However, they usually can be left in situ. Patients can usually be mobilized immediately postoperatively. The sutured bandage and stent are removed completely on postoperative day 5. After this, the neovagina is flushed daily with a saline solution, and compresses saturated with ointment are inserted. A combination of enzymatic and antibacterial ointments is recommended. The indwelling urinary catheter can be removed as soon as the urethral meatus has fully healed.
Dilation is begun once the wounds in the neovagina have stabilized. This is done with various sizes of foam rubber stents, which are given to the patient for use at home (▶Fig. 6.6). During their stay on the ward, patients are gradually familiarized with their new anatomy and with appropriate wound care. They are only released when they demonstrate their ability to clean the wounds, including vaginal douching, dilation, and insertion of the spacer. The average stay in the ward is about 14 days.
6.2.9 Aftercare
Thorough aftercare by the patients themselves is crucial to achieving good long-term results. To avoid scarring and shrinkage of the vagina, patients must be instructed to dilate the vagina at least three times a day for a period of 6 months and then to douche, or to consistently insert a spacer. After the wounds have completely healed, the ointments used initially can be replaced with ointments containing panthenol and estrogen (▶Fig. 6.7, ▶Fig. 6.8).


6.2.10 Corrective Surgery
Patients should be offered the opportunity to have the surgical result optimized only 6 months postoperatively at the earliest. Optimization focuses primarily on the following aspects: the erectile tissue of the inverted urethra is often clearly too prominent at the introitus, especially when the patient is excited. Reduction of the corpus spongiosum is indicated in such cases. The posterior commissure of the vaginal introitus is often too narrow and can be expanded with a simple V-Y plasty that shortens the perineum. Other common complaints include folds of excess skin (often referred to as dog ears) on the labia majora that can be resected. If necessary, corrections can be made to the urethral meatus if the stream of urine deviates, or labial asymmetry can be addressed (▶Fig. 6.9).

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


