6 Preoperative Clinical Evaluation of Patient
Summary
A preoperative overview for nasal septal perforations requires both an anatomical local evaluation and specific diagnostic test. The assessment begins with carefully assessing patient’s medical history. The physical examination starts with the inspection of the nasal pyramid for any alterations regarding the structural deficit. The nasal endoscopy allows the definition of the size and site of the perforation. The septum should be palpated with a sticker or with a cotton-tip in order to discern persistent cartilage between mucosal flaps and to determine whether cartilage extends close to the edges of the defect. CT scan with bone details can provide information about the structure of the residual septum and quantify the exact measurements of bone/cartilage defect. Lab tests should also be considered.
The causes of nasal septal perforations (NSPs) are numerous and can be either related to local or systemic conditions. Therefore, a preoperative overview requires both an anatomical local evaluation and specific diagnostic test.
It is essential, before proposing any surgical treatment, to clarify the etiopathogenesis of NSP.
The assessment begins with assessing the patient’s medical history carefully. Patients may present the major symptoms of NSP, such as crusting, bleeding, whistling, nasal obstruction, and, sometimes, pain and rhinorrhea. It is necessary to investigate the onset of the NSP and any previous intranasal procedures eventually associated with septoplasty, and septal cauterization for anterior epistaxis. The possibility of septal damage can be linked to particular events, such as trauma, cocaine, nasal foreign-body injuries, and decubitus by nasogastric tube.
Some patients’ habits can be considered, such as excessive use of nasal decongestants or topic steroid, and frequent digital trauma to remove intranasal crust. Finally, some risk factors related to occupational exposure, such as chemical irritants, and to specific diseases, for instance tuberculosis or syphilis, should be investigated. 1
The physical examination starts with inspection of the nasal pyramid for any alterations regarding the structural deficit. Indeed, large NSP can result in loss of support of the nasal dorsum and consequent “saddle nose,” sometimes associated with a deviation of the caudal edge of the septum. The nasal endoscopy with rigid fiber optics (30 degrees) is a key step of the physical examination. The use of topical decongestants and local anesthetics can make it easier and tolerable, especially in cases where the removal of crusts by an underlying mucosa, easily bleeding areas, or a biopsy is expected.
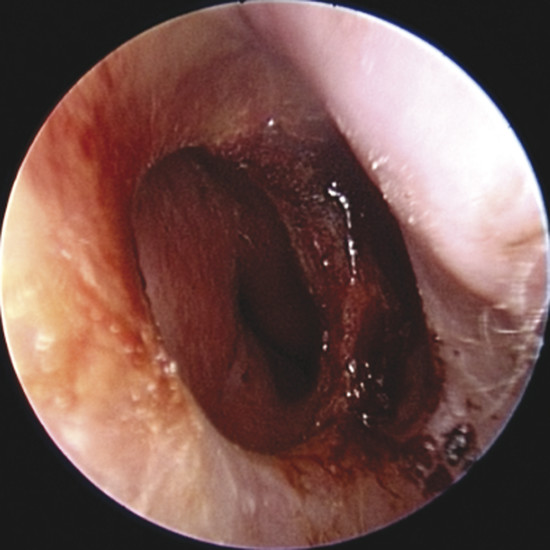
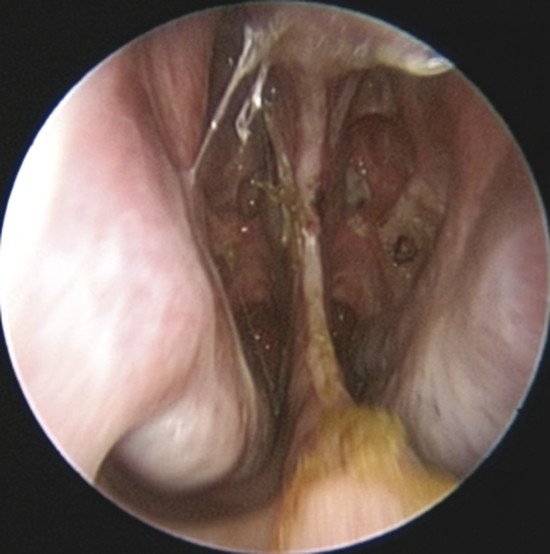
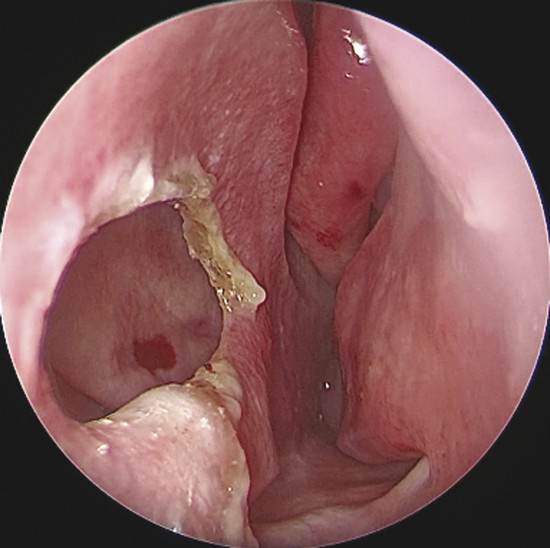
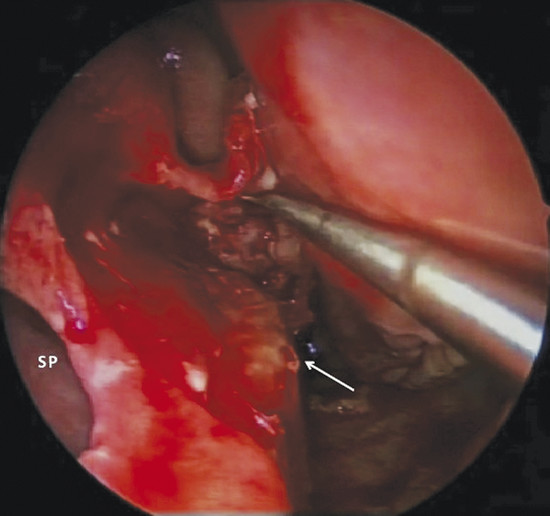
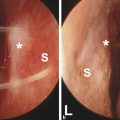
Upon physical examination of the nose, a full diagnosis cannot be made until all crusts have been removed and decongestion of the turbinates has taken place, making it possible to visualize the entire nasal septum. The nasal endoscopy allows appreciating the configuration of the NSP, the presence or absence of adherent crusts on the edges of the defect (Fig. 6‑1), any easily bleeding areas (Fig. 6‑2), and the state of the remaining mucosa, which may present some aspects regarding ischemic conditions (cocaine abuse) (Fig. 6‑3).

In addition, it is possible to measure the size of the NSP under endoscopic control that is critical when choosing the most suitable surgery (Fig. 6‑4).
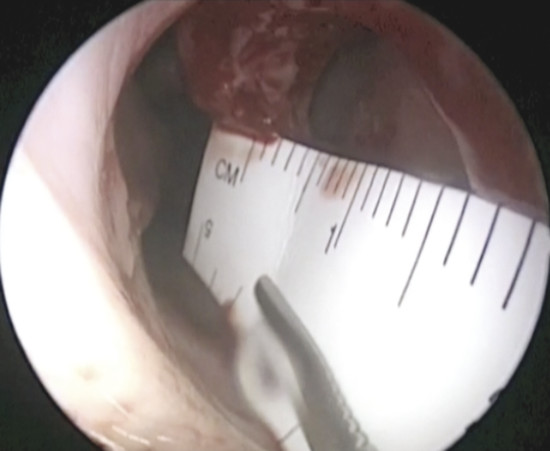
The measurement of the defect can be performed in several ways.
The disposable paper ruler found in some surgical pen packs can be trimmed and introduced into the nose to obtain an accurate measurement. If this instrument is not available, the graduated end of the Cottle septum elevator can be carefully inserted and slid against the septum to determine the size of the NSP.
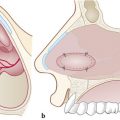
If the defect is not circular, but oval in shape (Fig. 6‑5), it is appropriate to obtain an exact measurement of the major diameters: anteroposterior and craniocaudal, vital in choosing the most appropriate surgical technique. The vertical height of a perforation has been predicted to play a more important role in determining the surgical success than the horizontal length because the main tension between the floor of the nose and the dorsum was critical. 2 The final aspect that must be considered for surgery is the location: anterior, posterior, near the floor, or in the cranial part of the septum. Septal spurs must be identified during endoscopic examination. These should be removed during flap harvesting to get one more large and flexible mucosal layer. (Fig. 6‑6). The septum should be palpated with a sticker or with a cotton tip to discern persistent cartilage between mucosal flaps and determine whether cartilage extends close to the edges of the NSP. 2 In perforations that have occurred after septoplasty, there is usually very little cartilage left, and this makes dissection of the flaps more difficult. In this phase it is also important to check the quality of other intranasal anatomical structures, which represented potential donor sites of grafts or flaps, such as the inferior turbinate, the middle turbinate or the floor of the nasal fossa.
Often, the size of the bone or cartilage defect may be greater than the mucosal borders of NSP. Therefore, a radiologic investigation such as a computed tomographic (CT) scan with bone details can provide information about the structure of the residual septum and quantify the exact measurements of bone/cartilage defect. CT scans can also show any inflammation coexisting at the level of paranasal sinuses.
In patients without a likely local cause for the NSP or in patients with rheumatologic complaints, basic laboratory studies may be performed.
The rheumatoid factor (RF) level may be elevated in patients with rheumatoid arthritis, mixed connective tissue diseases, lupus, scleroderma, or other disorders. Elevated angiotensin-converting enzyme (ACE) levels can indicate the presence of sarcoidosis. Chest radiography can also be performed to assess mediastinal lymphadenopathies.
Churg-Strauss syndrome is characterized by increased levels of antineutrophil cytoplasmatic antibodies (p-ANCA) and eosinophilia. Wegener’s granulomatosis is often associated with increased levels of antineutrophil cytoplasmatic antibodies (c-ANCA), erythrocyte sedimentation rate (ESR), and RF, but these are less specific indices. 3
If any of the results are positive, consult a rheumatologist regarding further investigation.
For patients who use cocaine, it is absolutely mandatory to identify whether cocaine catabolizes in urine, or if possible, from hair. These patients must sustain or cease cocaine use at least 1 year prior to performing surgery. These patients should undergo periodic endoscopic controls to perform a toilet of the nasal cavity and remove the crusts from the edges of the perforation to prepare the surgical field. Moreover, instillation of drug emollients and antibiotic ointments are indicated.
In case of active and inflamed lesions of the septum around the mucosal edges of the perforation, a biopsy should be performed. The tissue can be sent for histopathological examination to exclude neoplastic lesions as well as for fungal and acid-fast bacilli cultures.
Biopsies of the superior edge of the NSP should be avoided because they contribute to increasing the craniocaudal diameter as well as the difficulty in the surgical repair. 4
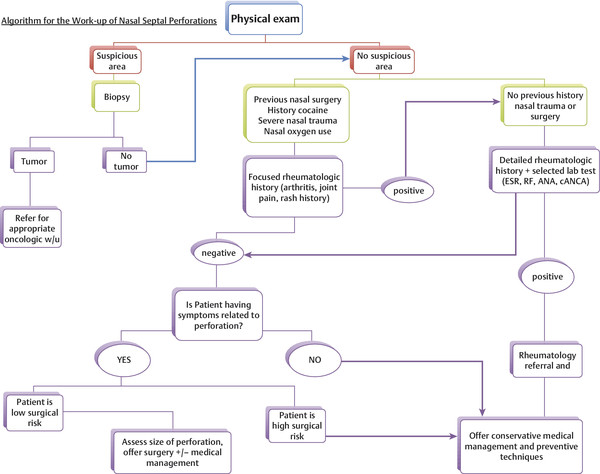
Batniji in 2012 proposed an algorithm for the preoperative evaluation of the septal perforation, 5 which is shown in the flow chart in (Fig. 6‑7)
6.1 References
[1] Kridel RW. Considerations in the etiology, treatment, and repair of septal perforations. Facial Plast Surg Clin North Am. 2004; 12(4)435–450, vi [2] Kridel RW. Septal perforation repair. Otolaryngol Clin North Am. 1999; 32(4)695–724 [3] Diamantopoulos II, Jones NS. The investigation of nasal septal perforations and ulcers. J Laryngol Otol. 2001; 115(7)541–544 [4] Watson D, Barkdull G. Surgical management of the septal perforation. Otolaryngol Clin North Am. 2009; 42(3)483–493 [5] Batniji RK. Septal Perforation—Medical Aspects Treatment & Management. Medscape Reference Feb, 2012. emedicine.medscape.comRelated posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


